
3/30/24 – I have updated this post to provide a preamble, bullet points, of what this article is about. The article itself goes thru the science backing these bullet points, including various published papers, and the description of how a body can be effected – naturally and/or via induced reactions. Deterioration can be either rapid or slow. It explains why doctors may never suspect the underlying cause using basic testing and years of fixed assumptions. There can also be a genetic link to which doctors have never been exposed.
Let me start with a quote from a paper that lead me to connecting a wide range of dots:
“Despite of multiple advantages of this system in biotechnology, further research is required to understand the immuno-toxicity of the avidin and its variants.”
The quote is taken directly from the paper: The Principles and Applications of Avidin-Based Nanoparticles in Drug Delivery and Diagnosis by Akshay Jain and Kun Cheng
I also perform my research under the guidance of an Occam’s Razor Explanation of Disease. This concept follows the thought that the simplest answer (connection) should be considered first. There is actually ONE connection that can tie together all “disease” and “side effect” pathology – BUT – there are multiple contributing factors to it that no one would ever suspect so they dismiss the premise at face value.
- A large majority of Medications and Vaccines are delivered to cells via a process called Biotinylation.
- Drug nanoparticles are coated with Biotin (natural or a preferred bioengineered form) in order to “fool” the cell to accepting it inside. (it’s the Trojan Horse) This also pertains to LNP – Lipid Nano Particles and even treatments such as monoclonal antibodies.
- A protein called Avidin (natural or a preferred bioengineered form) is used as the delivery method that safeguards the Biotinylated drug particle until it reaches its destination.
- If Avidin were to be consumed or injected on its own it would be considered a neurotoxin because it will bind Biotin within a body and render it unavailable. This can cause cellular collapse but yet be undetectable via normal testing. The above mentioned paper states that it is known some forms of Avidin are more immunogenic than others.
- When Biotinylated drug nanoparticles are chemically “disconnected” from their Avidin delivery method (via reagents like PEG and others or natural displacement with free Biotin), the Avidin protein can then grab “free natural Biotin” from the body and render it useless. This could cause an immuno-toxic and/or neurotoxic effect, sudden or gradual, that would compromise the body. In people who can unsuspectingly carry a gene that can lower the body’s ability to “recycle” Biotin by 50% (Low Functioning Biotinidase) – it can be catastrophic. (Bioengineered Biotins may not function and recycle like natural Biotin meaning loss of “free natural Biotin” could lead to cell apoptosis or dysfunction.)
- Egg white contains Avidin. Symptoms from consumption of raw egg, caused by Avidin binding of Biotin, is HOW Biotin was discovered as a Critical nutrient. The disease “Egg White Injury” was coined in the 1940s as a result.
- The Avidin protein is now being genetically inserted into grain crops. A form of Avidin protein known as Rhizavidin is found naturally within the “common bean” we eat every day. (raising everyone’s risk of inducing undetectable slow Biotin deficiency and could be the link to gastrointestinal issues)
- MANY blood/urine tests that measure Critical protein/hormone/enzyme/vitamin levels use a method called Avidin-Biotin Assay. The FDA has issued a warning that high supplementation with Biotin could then affect testing level outcomes. (not all doctors even understand this) However, the FDA has never stated that deficiency of Biotin could also affect these same outcomes. Biotin levels are essentially never tested and no one would test a body for the possibility of excess Avidin infiltration even though it is used in common medications and can be consumed in diet. If a body is not tested for a “control” amount of Biotin – there is no way to understand if a test result is actually reflecting a Biotin induced issue. A Biotin functioning issue could actually be the cause of disease.
- Biotin deficiency via any cause or combination of circumstances can induce Functional Deficiency of B12 as Adenosylcobalamin in the Mitochondria. (Directly Inactivating, turning off, the cell’s ability to create Succinyl CoA – ATP) This can create “mitochondrial dysfunction” and can lead to “protein misfolding”, DNA/RNA corruption and other related issues. Without producing Succinyl CoA it will also lead to reduction in heme – a precursor to hemoglobin – leading to oxygenation problems. The inability to create ATP can inhibit the body’s ability to create hormones/proteins/enzymes and even things like Vitamin D or CoQ10 and others – all created inside the body. It also can prevent the removal of toxins and cause a dangerous elevation in metabolites. Theorhetically this could even be the connection/explanation to induced autism.
- Beta-Hydroxyisovaleric Acid should be part of any Testing Protocol – especially in the case of any difficult diagnosis in particular involving a “neurologic issue”. (This is now an accepted sensitive Biotin functioning indicator and known to elevate after an “Avidin event”- like toxin/chemical ingestion/injection – or even in those who smoke or may be exposed to toxic chemicals) Another indicator for testing could be Propionic Acid which is a pre-cursor to Biotin metabolism – elevation could then indicate Biotin insufficiency to process. Propionic Acidemia is actually a known listed side effect of some pharmaceuticals. Propionic elevation can cause breathlessness in patients as toxins build and oxygenation falls and may cause stomach distress and vomiting and lethargy among other symptoms.
- Serum B12 levels are an extremely INACCURATE method to test B12 until such time as deficiency becomes dangerously low and levels show up in the “low normal” range. Because Biotin deficiency causes Functional Deficiency of B12 in the mitochondria (an inactivation and interruption of the B12 cycle), serum B12 levels can be falsely elevated within the entire “accepted normal” range, and can often show up as levels exceeding high normal. When B12 is being supplemented serum ranges will essentially never be accurate. MMA (Methylmalonic Acid) is another indicator of B12 after Biotin metabolism, but needs to be tested as both serum and urine (kidneys flushing blood) to gauge and used in conjunction with Biotin testing to know if Biotin deficiency is influencing its levels and causing it to appear in the normal range.
- Biotin deficiency has been researched to be a link to the inability to regulate cytokine function. Cytokine dysregulation has been a big factor in current pandemic diseases and side effect management.
- Glyphosate (the herbicide) is meant to disrupt the Shikimic Acid Pathway found in plants and bacteria. The first step in the shikimate pathway is a Biotin dependent enzyme. While it is known that glyphosate affects gut bacteria in humans and animals – the Avidin-Biotin delivery system could then explain additional connections made to toxicity and cancer for humans and animals due to Avidin residue on vegetation.
- If you believe a “Vitamin” cannot be critical to disease or recovery – please understand that the antidote for Cyanide poisoning (a neurotoxin) is Vitamin B12 in the form Hydroxycobalamin.
If any or all of these points are new to you as a doctor, researcher or patient, then the rest of this article contains further information that elaborates and expands on these facts. I also explain how I came to understand the connections from personal observational experience.
(Things Every Neurological Disease Patient Should Know)
Watch any TV commercial for a medication and you will hear the disclaimers for potential issues and side effects. In fact, you can hear many of the exact same possible side effects for totally different medications. The same reactions can happen in humans and animals. The answer may be because they all can have one thing in common, not the drug, but the way they are bio-engineered to be delivered to the cells of the body.
A few years ago I went searching for answers to neurological issues my dog was having, wanting to know what makes the body, human and animal, fail to protect itself the way it normally would. In the end I learned specific nutrient deficiencies were at the heart of her issues and why doctors don’t recognize the signs. I wrote a very long article to help others as I was stepping through what worked and what didn’t. Three years later and I have kept on researching because I saw similarities in her symptom progression not only to that of other dogs in Social Media groups, but even to progression in humans and especially babies. Both animals and humans are having reactions, in particular to vaccines, but also to general medications. From my research I knew that the reactions could all be related to one thing, but how were they all causing stress on this one pathway when each drug was different? Then I discovered one connection. The vaccines and medications aren’t the same, but there can be one common denominator undermining the body that no one recognizes and no simple blood panel will ever show.
I need to describe some particular nutrients in order to explain their connection to the side effects that are being experienced in both humans and animals. The vaccines and medications can be compromising these critical players, building blocks of other reactions in the body, so I want to elaborate on their functions. My research revealed that most doctors and veterinarians, including neurologists, really have no FULL knowledge of how these elements work and how they can become deficient or inactive – even when a test result appears normal. The first few paragraphs may therefore seem a bit irrelevant, but I want to provide some science before getting into how that information is used and effects the body, so please bear with me. I will then describe how and why this can be happening, breaking down the body, along with additional details in specific areas that can explain why doctors may be dismissing things too soon and not exploring all testing elements. This won’t be a short explanation, but to be thorough it cannot be concise. I also want to provide as much information in one place for people who have never been exposed to this level of detail on these nutrients, in particular their relation to neurological issues and disease progression like ALS or other autoimmune reactions, and even DM and other diseases in dogs, in case it can help any person in the quest for their own answers. Only a patient may know if they fit into these descriptions of how their body began to break down, things they suspected all along that a doctor disregarded.
During my research I educated myself on everything B12, one of the critical neurological players in the body. It is also a key to blood cells, both red and white and platelet and cancer fighting cells, a cornerstone of DNA and RNA, and a critical nutrient in fatty acid metabolism. Virtually every chemical reaction in the body is associated in some way with B12 – either directly or as an end product of B12 functions. B12 deficiency and inactivity is also a known player in the destruction of nerve cells called demyelination that leads to nerve cell death. It is also a cause of Spinal and Brain Atrophy. Just that one vitamin works in so many different ways that doctors don’t even understand how it can be connected to various issues and symptoms because they are typically trained in only one way to look at it and even to test it. Most can’t tell you that it works in the body as Methylcobalamin AND Adenosylcobalamin, a very significant factor, they simply know it as B12 or cobalamin. They do tend to believe a body doesn’t easily get deficient because we have “storage” – but that storage is actually in the form of Adenosylcobalamin in the cell Mitochondria – the most prominent source in the body – and the most “untested” form of B12. I will forego that science right now. Doctors do however usually know that if you are a declared vegetarian, or in particular vegan, that you are at higher risk for B12 issues because it is only found in meat, seafood, eggs and dairy. The cells of those foods provide both the Methyl and Adenosyl forms of B12 to the body. The problem however is that evidence has been increasing that B12 deficiency is affecting a larger amount of the population than previous thought, including children and especially seniors, even animals. Researchers have identified that children with autism are found to be functionally and overall deficient. A large amount of seniors, especially those with cognitive impairment, Alzheimer’s or Dementia, are also found to be functionally and overall deficient. Functional deficiency is when a standard Serum B12 blood test can be normal, high normal or even high (in particular levels exceeding 700), but yet the body has clear B12 deficiency symptoms – mostly neurological including psychological. Overall deficiency is Serum B12 levels that are low normal or below normal. People are becoming more educated and requesting thorough testing and, when interpreted properly, which is not always the case, are finding underlying deficiency as the cause of their symptoms. However, the problem is that doctors in general DO NOT understand “functional deficiency” and are dismissing the neurological signs based upon Serum B12 levels.
This article may be of interest, it describes other B12 markers and some facts that may enlighten both patients and professionals. But, it still does not tell the whole story because it does not address “high” B12 levels, nor hidden contributing factors. Vitamin B12 – The Reference Range Level is Set too Low https://mthfrsupport.com.au/2015/03/vitamin-b12-reference-range-level-set-low/ The Many Faces of Cobalamin (Vitamin B12) Deficiency https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6543499/?fbclid=IwAR0hTWPMw1o0cH6LuvCqAZVXm--s-cqQxrkmJCDytQ936twH1a3yLS66oss#!po=0.438596 Serum B12 test is often not sufficient to diagnose a deficiency https://stichtingb12tekort.nl/english/the-serum-b12-test-is-often-not-sufficient-to-diagnose-a-deficiency/?fbclid=IwAR2_ByrNE_gne2ftPIm91bVbxlCnPy4rQB3jYll7XeSGTRdrfzhMe3sfXhg
B12 was at the heart of my dog’s issues, but I had to keep investigating even more when supplementation only worked for so long. B12 works indirectly with another key misunderstood and underestimated vitamin called Biotin. If Biotin is deficient it can cause B12 to become inactive in some of its critical functions – functional deficiency – and to eventually become overall deficient in the body. But, it is “largely assumed” that deficiency of Biotin would be a rarity – for humans and for animals. In fact in pet food manufacturing in the US, Biotin is not even a required nutrient by AAFCO in dog food. To be fair, it is “assumed” that the nutrient is available in the raw ingredients and that the heavy processing won’t destroy all of its availability. However, in humans at least, there is also a “genetic issue” that can come into play with Biotin that doctors would never even suspect could be an underlying agitator to deficiency – I will describe that issue in a few moments. Biotin does more than just interact in a metabolic pathway with B12. It is a significant player in other critical chemical pathways in the body. Deficiency of Biotin would then compromise not only fatty acid metabolism with B12, but that of carbohydrates and amino acids (proteins) and critical CO2 processing. Since Biotin deficiency can initiate functional B12 deficiency, long before it fully influences overall B12 deficiency, it has been noted that the first symptoms of Biotin deficiency can more readily increase neurological and psychological issues.
In the bio-engineering world, they now rely heavily on a facet of Biotin and its attraction properties to another protein. In fact, they exploit it to deliver medications, antibiotics and vaccines to the body. It is even a critical player in chemotherapy and contrast imaging drugs. It is even used in numbing agents like Novocain for dental procedures. It is also the basis of many medical testing procedures in extracting hormone and enzyme levels from blood and tissue samples – ironically – even to test B12.
Biotin has a kind of nemesis. Though really it could be called a love hate relationship of sorts. It has a practically unbreakable attraction to a protein called Avidin. This attraction has been called “one of the strongest non-covalent interactions in nature”. That attraction means that once bound together naturally, Biotin is then unavailable to function inside the body and will eventually get excreted.
Avidin is found in egg white. It was discovered in studies as far back as 1916-1927, that if egg white was consumed raw/uncooked or even undercooked on a somewhat regular basis that it would eventually lead to skin and neurological issues like ataxia, trouble walking. In the 1940s this was identified and categorized as Biotin deficiency – THIS is how Biotin was discovered as a critical nutrient. Though, in any one patient, human or animal, Biotin deficiency can be the basis for numerous other health issues long before the more severe neurological manifestations become apparent. Things like unexplained skin rashes or hair problems, hormone abnormalities and endocrine issues, gut problems, IBD/IBS, pancreatitis, glucose tolerance, swallowing issues, fatigue, muscle weakness, headaches/migraines, neuropathy like tingling sensations, pins and needles feelings, and even psychological issues or memory problems. These symptoms can stem from Biotin deficiency and its subsequent inactivating of critical B12 functions, along with other crucial functions in which Biotin participates. Biotin deficiency is even directly tied through its metabolic interactions to many forms of yeast infections, an extremely prevalent skin condition in dogs. It has also been tied to conjunctivitis (pink eye), a very prevalent eye infection in humans.
The Biotin deficiency occurs when whole eggs are usually consumed raw or simply undercooked in general like in adding them to protein drinks (smoothies) or ice cream shakes (my mom did this for us as kids), very soft boiled or sunny side eggs when the white is still very runny, Egg Nog made with whole eggs (a much consumed winter holiday drink that could then magnify risk factors, possibly the link to increased holiday disease and heart attacks – some egg nogs are made with just yolk, depends on recipe) or excessive consumption of mayonnaise and even uncooked meringues can pose a risk. Body builders have come to understand that drinking raw eggs like in the movie Rocky is NOT a good thing. After initial discovery it became known as a condition called “Egg White Injury”. It doesn’t happen overnight, but rather over a period of months or even a year or more depending on the body and how often consumed, so it is virtually impossible to see the direct connection. In a way it could be considered much like a slow acting poison whose affects build on the body over time. Just like cigarette smoke or other drugs, alcohol, mold or toxins in a home. It can go essentially unnoticed if the doctor isn’t astute to the condition or if the right questions aren’t asked of a patient because there is no easy direct testing method for Biotin deficiency, it is not an obvious marker on any standard blood panel, and because No One believes it can exist to any “critical” extent, but the danger may be in the “lesser” extent. The misconstrued thought is that it takes consumption of large amounts of raw egg white in a short time frame to do damage. Believing that it is safe to consume continual small amounts, maybe a raw egg or two a week, as can be done in the animal world, can actually be more dangerous. Quantity is a definite issue in short term effects, the problem and danger can come from missing the “lesser” longer term effects – especially if there is an unknown factor at play in the body – the basis for this article. Even if you don’t consume raw egg white knowingly, you can still consume Avidin. There are now some markers that can be tested to give a better indication of how Biotin is functioning, but it is a rare occurrence to test them. B12 functionality and levels eventually become effected, so understanding how to interpret them properly, IF they are tested, becomes more important. But in early symptom progression, Serum B12 levels may actually be completely normal – even high normal or high – Fooling everyone.
I will add a touch of scientific data to explain the Avidin-Biotin attraction. One regular chicken egg is stated to have approximately 180mcg of Avidin, it can have more. That same egg has approximately 30mcg of Biotin. Avidin binds Biotin at a rate of 1 part Avidin to 4 parts Biotin. So that 180mcg of Avidin can bind 720mcg of Biotin (180×4). That is the ability to bind to 690mcg extra of Biotin in the body (720 minus 30) when consumed as a whole raw egg and render it useless. That figure far exceeds the recommended human minimal daily intake of Biotin by over 2,000%. And Avidin is only deactivated of its attraction when cooked at temperatures above 185 degrees Fahrenheit for 3 minutes. So neither freezing, freeze drying, dehydrating, nor stomach acid will stop its attraction, making it very appealing to bioengineers. It has been suggested that pasteurization denatures Avidin, however, pasteurization temperatures are lower than the known deactivation temperature. Pasteurization is only meant to kill bacteria. Avidin is a protein and not a living organism like bacteria. Therefore it should not be assumed that pasteurization of eggs or egg products renders the Avidin safe for regular raw consumption.
This description of Avidin was taken directly from a pharmaceutical https://bioseutica.com/products/avidin website:
A highly basic glycoprotein tetramer, each AVIDIN protein is an assembly of four identical subunits composed of 128 amino acids. Each of these subunits binds to Biotin (Vitamin H, Co-enzyme R, Vitamin B7) with extreme affinity, in the order of 10,000 to 10,000,000 times the strength at which an antibody binds to its antigen 1.
This biotin-binding by AVIDIN is not only strong, specific, and rapid, but resilient too, withstanding proteolytic enzymes and extremes of temperature and pH. These properties, it being one of the strongest natural non-covalent bonds identified, has made the AVIDIN-biotin system extensively employed across the biotech industry.
AVIDIN’s discovery came from the observation of ‘egg-white injury’ in animals fed a diet rich in raw egg-white. Symptoms resembling Biotin deficiency, despite the dietary sufficiency led to the identification of AVIDIN as the component that was rendering Biotin unavailable. For the egg, the source of AVIDIN, this function is a key line of defence in its nutritional immunity, similar to the iron-sequestering role of OVOTRANSFERRIN.
Most organisms other than plants and a few micro-organisms are unable to synthesise Biotin for themselves, so are heavily reliant upon these sources for their continued supply. This relative rarity in nature makes it precious, as Biotin is a key co-factor of enzymes critical for central cellular metabolic processes. By making the egg-white a ‘biotin-free zone’, AVIDIN starves invading organisms of this co-factor, binding all free Biotin to render them incapable of proliferating. This capability is potent, despite AVIDIN comprising a mere 0.05% of the total protein of the egg-white (a trace 1.8g per egg).
Let us take the above fact even further:
The Avidin Gene is now being introduced into wheat crops. This is done to prevent damage from insects during storage – the “killer” is INSIDE the wheat. If the wheat is also sprayed with glyphosate to desiccate it during storage (one way of preventing mold and other bacteria), it could technically be considered even more toxic. The following study proved not only that Avidin protein was built up in genetically modified wheat, but that it transferred into the insects. This would mean that the very same thing could happen in humans and animals consuming these products. The reaction would not be immediate like in the body of an insect. However, with constant consumption of “grain products” (breads, cereals, crackers, cookies, pasta, pizza dough, or anything that uses wheat flour in its production) – every “Being” would be at risk for induced Biotin deficiency as the Avidin protein is constantly introduced back into the body. As of this writing I do not know if this genetic process has been introduced into other plants or grain based flours, but it is likely the next step.
https://pubmed.ncbi.nlm.nih.gov/26194497/
1985- LITTLE-KNOWN BIOTIN ONLY GETS NOTICED WHEN IT`S NOT WORKING https://www.chicagotribune.com/news/ct-xpm-1985-05-23-8502010903-story.html
Why is this important? Because bio-engineers are using the attraction between Biotin and Avidin to bind drug nanoparticles and deliver them to the cells in the body. The Biotin pathways in the body have been used extensively for drug delivery for quite some time, but this Avidin-Biotin binding process has increased exponentially in the past few decades because it helps to stabilize drugs. They have even created various strains of Avidin in order for them to react differently in the body and direct drugs easier to certain areas. One such Avidin variant is called StreptAvidin, but there are more. They coat the drug particles with Biotin (this is called Biotinylation) and they can then attach them to Avidin to protect them and deliver them to the cells. Each drug company would use some proprietary method to do this, and a proprietary method for how the particles are able to detach once inside the body and cells – it all depends on the nature of the medication or vaccine and the metabolic pathway they are affecting. Actually, some of the unusual and controversial ingredients that may be listed on a medication or vaccine, such as polyethylene glycol (PEG) and others, are called “reagents” and used for this very process. The Biotinylated particles are then absorbed into the cell and into mitochondrial function of the cell to alter proteins, enzymes and antibodies the cell may make so that it can affect the reactions the body is having. Since Avidin and Biotin are considered natural ingredients, you likely will not see them listed on any label – but you will see side effects listed than can give you a clue that the Biotin pathway is being disrupted.
This article from NIH explains the myriad ways that Avidin is used in bioengineering. The Principles and Applications of Avidin-Based Nanoparticles in Drug Delivery and Diagnosis https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5222781/
This article from the Journal of Immunology discusses a method of increasing cell replication. If this process is used in vaccines or antibiotics to induce faster action in the body it could further strain the system resources increasing the side effects from deficiency. VaxCelerate: the use of MTBhsp70-avidin as an adjuvant to rapidly generate self-assembling vaccines with biotinylated, antigen-specific peptides targeting emerging pathogens. https://www.jimmunol.org/content/192/1_Supplement/140.2 The journal has recently removed this article link but it can be found at the following link: https://www.semanticscholar.org/paper/VaxCelerate:-the-use-of-MTBhsp70-avidin-as-an-to-Fishman-Moise/c229bf0213cb8a6fbcb258bbee29fb2194068aed
There is a Non Egg White white variant of Avidin that has been found in the Common Bean that is a staple in many human diets and is often used in animal diets – the common bean covers many variations of plants/types. This Avidin variant is called Rhizavidin. Though slightly different in structure, it appears to have the same Biotin binding affinity as StrepAvidin and Avidin and the ability to process in the liver. One more way Avidin can be consumed on a regular basis without knowledge. Rhizavidin from Rhizobium etli: the first natural dimer in the avidin protein family https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2267316/
Biotinylation Explained – https://www.thermofisher.com/us/en/home/life-science/protein-biology/protein-biology-learning-center/protein-biology-resource-library/pierce-protein-methods/biotinylation.html
This bioengineering is not a sinister plan, but an extremely efficient way of getting lifesaving drugs to cells, or even to contrast areas of cancer when doing a CT or MRI. For antibiotics it can mean the difference between halting a bacterial infection or it ravaging a body till death. Drugs have indeed saved lives. But at the same time, because so many different Medications and Vaccines are using the Same Metabolic Pathway, it could also be causing an Issue No One Is Recognizing. You can compare it to rush hour traffic – everyone uses the same road(s) to get to and from work – it can then lead to accidents, traffic jams, or simply to roadway deterioration from overuse. We may be beating up the Biotin pathways and consequently not understanding the potholes we have created.
There is also a strong possibility that after a vaccine or medication is delivered to the cells and unbound from Avidin, that the Avidin protein then has the ability to bind to free Biotin and remove it from the body. To what degree is based upon the amount of Avidin in the dosage of the vaccine or medication. Extended Release medications may in particular use this method since the Avidin binding would protect it and utilize chemical reactions that would allow it be broken down further within the intestinal tract – allowing Avidin to remove free Biotin directly from within the gut. If there is a chance that a body is already moderately deficient in Biotin, or has an unknown underlying genetic issue with recycling Biotin (biotinidase issues), the Avidin could remove a dangerous level of free Biotin and affect cell function, including critical B12 functions and cell signaling. The cell would also likely not be able to filter and remove toxins if impaired. Biotin is a critical player in CO2 functions in the body. If more than one vaccine or drug is administered at the same time, in theory, it could indeed be deadly. Not just for potentially removing free Biotin, but also for the overload on this one particular metabolic pathway which can prevent normal recycling of Biotin due to chemical alteration. Repetitive medication consumption could then affect the Biotin pathways and continually rob the system of free Biotin without gut bacteria being able to produce enough replacement and get it in circulation, nor the diet being able to resupply enough. The realization for this came from a friend who has RA (rheumatoid arthritis) and has taken medication most of her life. Many years ago she discovered that the only way to prevent her hair from falling out was to take an increased dosage of Biotin. I now find that connection significant.
To prove what I have just stated – Thermo Fisher Scientific (in the above linked article to explain BIOTINYLATION) actually describes this very action/intent when explaining a type of biotin that has been created called Desthiobiotin. This is the text from the webpage:
Desthiobiotin
Desthiobiotin is a single-ring, sulfur-free analog of biotin that binds to streptavidin with nearly equal specificity but less affinity than biotin (Ka=1011M-1 vs. Ka=1015M-1, respectively). Consequently, desthiobiotinylated bait proteins and their interacting partners can be eluted readily and specifically from streptavidin affinity resin using mild conditions based on competitive displacement with free biotin.
In other words – the bio-engineering relies on the presence of FREE BIOTIN to break the weaker bonds on the manufactured biotin that is carrying the “drug”. Avidin binds the free biotin and would then render it unavailable to the body. As I stated above – this could, especially in a genetically compromised body, create a circumstance that destroys cells (if the medication using this method is concentrated in an area like through an injection), or lead to long term issues (if the medication is given via IV or through oral form that enter the GI tract allowing it to remove free biotin directly from the gut where it is released from food or produced via gut bacteria and is supposed to travel throughout the body including directly to the brain). If an oral medication is taken continuously – like long term diabetes or heart meds, etc. etc. – this can explain “side effects”.
A few years ago a relative had a Whipple Procedure for Ampullary Cancer, the same extensive and gut altering procedure as done for most Pancreatic Cancer. Her first symptom of cancer was almost complete liver failure due to duct blockage, the largest concentration point for Biotin and B12 in the body and the heart of fatty acid metabolism. The surgery actually removes the main digestion points for Biotin and B12. After surgery, before any chemo was started, but after an already enormous amount of medications and anesthesia (6+ hour surgery) and continual antibiotics to fight infection, her hair eventually began to thin, fall out, and her skin was excessively dry. She also experienced a great deal of mental confusion immediately following surgery and her body overall had trouble recovering, especially with fluid and nutrient balance and infection, and she seemed to have no sense of taste and even her sense of smell was effected. She had gastroparesis (stomach not working- a function of the autonomic nervous system), so the hospital finally gave her liquid nutrition via IV called TPN (Total Parenteral Nutrition). An interesting medical fact is that TPN use usually does not supply Biotin so it must be intentionally prescribed and added. (This exclusion of Biotin is likely intentional because blood tests use the Avidin-Biotin assay and extra Biotin could then cause inaccurate results. See my FDA WARNING section at the bottom of this article) After the TPN still did not improve her gastroparesis and overall state, they inserted a jejunal feeding tube to bypass the stomach and put nutrients directly into the intestine. Even the highly processed feeding tube formula (not real food) was not improving her gastroparesis nor appetite. Only when she was discharged from the hospital and then began taking organic liquid vitamins and an organic whole food feeding tube formula (Liquid Hope) plus some small doses of milk kefir to replace gut bacteria and a little collagen hydrolysate to provide readily absorbable protein, all put into her feeding tube, did her body finally start to recover. All supplied an increase of Biotin and bioavailable B12 in addition to a full array of critical nutrients in natural forms, good bacteria, and actual cells that the body could begin digesting to repopulate the gut microbiome after severe trauma and medication destruction. An interesting development in her recovery appeared a few months later – a small blood clot developed in the area of the surgery – an area that is targeted in repeated CT scans. I will discuss how clotting is a factor with Biotin in a few minutes.
If you look at the potential side effects of many medications and vaccines you can note possible symptoms to include the gastrointestinal system and neurological system including psychological issues, Guillain–Barré syndrome, liver and kidney issues or pancreatitis, acidosis, cancers/lymphoma, even heart problems, general muscle weakness. You may also see conditions such as skin issues or rashes, hair loss. Maybe even blood reactions or the possibility of clots. One interesting noted reaction for some medications is the possibility of interference with “lab results” – see the section I wrote on FDA WARNING below as this is a known issue with “biotin” and can further support the purpose of this article. There are a host of medications that have been directly linked to and with B12 deficiency. These include birth control pills, diabetes, arthritis, acid reducers (PPI), seizure, allergy, thyroid, pain, ADHD, anxiety and depression medication, just to name a few. If you do an internet search on any particular medication or condition and B12 deficiency, you may be surprised at what you find – research studies linking both. It is also important to mention that B12 actions are necessary to our sleep cycles. People usually only associate B12 with energy, but since it is critical to the chemical reactions necessary for sleep, Melatonin creation, deficiency can reduce the ability to fall asleep and stay asleep. Melatonin is created from Serotonin in the pineal gland but it is also produced in the digestive mucosal cells of the GI tract, making the GI tract the largest concentration point of Melatonin in the body. This is another reason why B12 has been connected to IBS/IBD and other GI tract issues. It is also connected to depression and anxiety disorders – the same conditions for which drugs are prescribed that focus on Serotonin levels. What happens in the gut is fed to the lymphatic system and up to the brain – hence the reason you have heard reference to the gut being the “second brain”.
But at the same time, because so many different Medications and Vaccines are using the Same Metabolic Pathway, it could be causing an Issue No One Is Recognizing. We may be beating up the Biotin pathways and consequently not understanding the potholes we have created.
In some cases, particular medications may even list that they can increase something called Propionic Acid. What you may not know is that some medications are even called a “Propionic Acid Class of Drug” because they utilize this metabolic pathway. One such major player is the pain reliever Ibuprofen (aka Advil/Motrin), for dogs it is called Carprofen (aka Rimadyl) – both known to cause liver and kidney damage with extended use.
All of the medication side effects can be linked back to Biotin and B12, the interference of and/or deficiency of these nutrients. Both of these have separate functions, but they do work together within the particular pathway called the Propionic Acid process in the body that metabolizes specific proteins (amino acids) and fats and cholesterol and uses them for cell energy called ATP. ATP is considered “energy currency” in the body because other chemical reactions need it to function. They are the key to critical fatty acid metabolism, brain function, organ and heart health, muscle, ligament and tendon health, blood and blood vessel health, nerve health, cell health, cholesterol levels, and on and on. This metabolism is turned into a type of fatty acid called Propionic Acid. Even our gut bacteria can naturally produce Propionic Acid. Interestingly, food manufacturers now use Propionic Acid as a preservative. It is coated on cheese and added to other items to improve shelf life. It is now even used in flavor enhancing. Our new obsession with fermented foods in both the animal and human world actually increases Propionic Acid too. Fermentation naturally increases the acid. There are even some scientific studies that are using Propionic Acid for treatment purposes to see if it will stimulate certain healing in the body. The acid is good under normal function, BUT, without enough supporting nutrients, namely Biotin, it is also dangerous if it builds. We essentially may be overdoing a good thing because we don’t understand it is only part of a bigger process.
A very simplistic explanation of the process is that when Propionic Acid is created (via processes that require and utilize one form of B12 called Methylcobalamin) it is taken by the body and combined with Biotin to make another acid called MMA (Methylmalonic Acid). MMA is then combined in a reaction with a different specific form of B12 called Adenosylcobalamin. There are many models that also make mention of Magnesium playing a role in this step. Deficiency of Magnesium can then also be critical to effecting this stage – conversely however, high serum levels of magnesium might indicate that this process is failing due to Biotin/B12 issues and should be investigated. This then creates cell energy, ATP. ATP is then used in other chemical reactions like creating hormones or other proteins, enzymes and fatty acids the body needs. After all, the body is just one big chemistry set of chemical reactions, many cyclical in nature – they initiate another reaction. For those who know the term Citric Acid Cycle, also known as Krebs Cycle, this is a major part of it. So if something is missing, the cycle can stop or at the very least, gets interrupted. Think of a car trying to run when it is low on fuel or oil, the car doesn’t have the ability to run smoothly as it gasps, sputters, to keep functioning properly. And if either is too low, the engine seizes or dies – there is a co-dependency. If there is a deficiency in either B12 (in both its forms) or Biotin, both of those acids can begin to build in the body and cause damage and begin to undermine the very functions that keep the body healthy, running smoothly. The body can make ATP through other chemical reactions, though Biotin deficiency can restrict some of those too, but this pathway is the most prominent and most critical, and without those acids being metabolized, disease can happen, and yes, death. The reason why some medications may specifically state that they can elevate Propionic Acid would likely then mean they are interfering with Biotin. Without Biotin processing the Propionic Acid you end up with “Propionic Acidemia” which in turn can lead to pancreatitis – a condition that is increasing in both humans and animals. Frequent pancreatitis could be the connection to increased instances of Pancreatic Cancer.
For a “visual” depiction of the process – use this link to scroll an NIH article on Methylmalonic and Propionic Acidemias https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5393914/
When babies are born, at least in most hospitals in the US, starting around 1984, they are usually tested for Organic Acid abnormalities because it is known to be life threatening and may not fully present for a few days or weeks after birth. These include Propionic and Methylmalonic Acidemia, the ones I described above. If they are not found to have dominant gene abnormalities related to these or other known acidemias, nor any elevation in these acids, essentially the medical profession never seems to think about them again. PA/MMA Acidemia are thought to be only neonatal diseases. Rarely are they thought of as a possibility of naturally occurring due to nutrient deficiency. This is in spite of the fact that some drugs are known to increase Propionic Acid, and in spite of the fact that MMA is known to elevate in B12 deficiency. Again, ironically, the only time doctors may check these levels is toward the final stage of disease, end of life. Elevation in MMA is usually considered a result of end stage renal failure and not always recognized as a possible cause due to nutrient deficiency, B12 deficiency, which can also cause the kidneys to fail. Other organic acids can also rise in deficiency of Biotin and B12. One called Beta-Hydroxyisovaleric Acid (aka 3-betahydroxyisovaleric) can be used as another marker for Biotin deficiency. When elevated it is a sign that Biotin is deficient and not completing other chemical reactions. It is known to elevate within approximately 5-7 days after an “Avidin” event – consumption or injection of Avidin, and is also known to elevate in smokers – meaning long term smokers are likely dealing with Biotin deficiency on a daily basis. There are also some case reports of “adult onset” of gene related diseases in regard to both B12 and Biotin. Biotinidase deficiency, primarily the inability to recycle Biotin (meaning a cell needs a constantly supply of free biotin else metabolic cycles can fail), is one of those rare issues that has had late onset in children and even teens and adults into their 20s – but only noted when it is Actually Tested for and recognized as a cause for symptoms, so instances could be higher. A person can carry a copy of the gene but yet function throughout life at a lower capacity until something happens that triggers a more profound downfall. They may have had a diet that included higher amounts of Biotin that compensated for the recycling issue or even taken a daily supplement that included increased amounts of Biotin to help compensate (daily supplementation of Biotin is the actual treatment for biotinidase deficiency). Then perhaps they changed their lifestyle and diet choices (like avoiding meat or organ meat), or maybe started a medication for something because of symptoms from the unknown underlying deficiency. Females may have started taking birth control pills, or teenagers may have started more intense sports to go along with their already stressed schedule, and it then triggered a larger system issue due to nutrient insufficiency. Just like a “cancer” gene can be triggered – so too could a sudden decline from a gene related to inefficient processes with B12 and Biotin. But if a patient is not fully tested for related metabolic imbalances when critical issues begin to arise, like severe neurological issues, one may never know if they are the trigger for a “disease” progression. A trigger like an overload/exploitation on one metabolic pathway that could lead to neurological collapse.
To give further example of how a gene can unknowingly cause issues, I can go back to my same friend with RA. A few years ago, when already in her 40s/50s, she had a general genetic testing done that gave her a list of various genes. I asked her if she could look at her test and see if it included anything regarding Biotin. Indeed it did, and it stated that due to a recessive mutation on one gene she is considered to have a 48% biotinidase deficiency. This would not be considered a profound deficiency, but under the right set of circumstances, could indeed be a trigger and become a profound issue. Like taking a medication that was affecting the Biotin pathway in her body – maybe robbing free Biotin. However, it does beg the question if indeed her “autoimmune” disease progression may have been induced by this issue all her life if her diet was not rich in Biotin sources or supplementation – creating her progressive disease. It was only after the medication triggered her hair loss that she discovered the “cure” for THAT symptom, but the damage had already been done.
This is the text from the genetic report in case it could be of help to anyone: rs13078881(G;G) common in ClinVar rs13078881, also known as c.1330G>C, p.Asp444His and D444H, represents a mutation in the BTD gene on chromosome 3. Inherited recessively, the rs13078881(C) allele is considered by ClinVar (and BabySeq) as a pathogenic mutation for biotinidase deficiency. However, it appears as if the D444H mutation results in 48% of normal enzyme activity, and if found in combination with a BTD gene mutation associated with profound deficiency, may result in partial biotinidase deficiency.
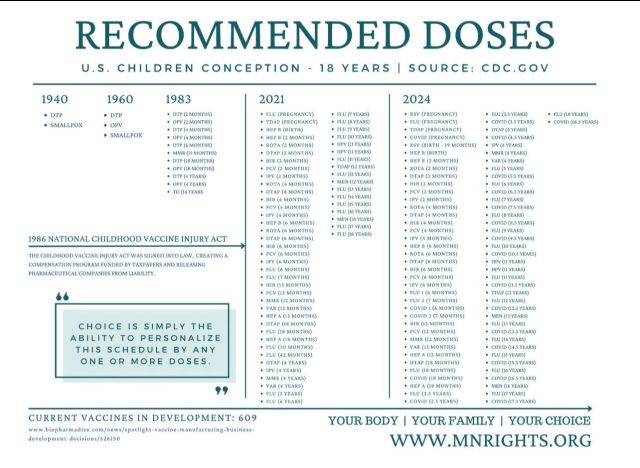
As a side note to this – I am attaching a chart I had found on the internet that depicts how the vaccine schedule changed in 1983 – the picture below depicts the requirement changes since 1940. I only now realized the correlation to the timing of testing on babies for Organic Acid abnormalities that started around 1984/5, that I mentioned above in relation to the increase in 1983. Did an uptick in “issues” that resulted from increased vaccinations create the need for this testing system? It may be plausible that although they knew profound genetic predilection can be an issue (Full blown Biotinidase Deficiency among others) – no one may have considered that recessive genetics, as in the notation listed above, could also present a problem. Meaning that, anything affecting Biotin recycling and creating or inducing a deficiency, could indeed create a symptom progression that would go completely unnoticed as to causality.
In some diseases you will hear about mitochondrial dysfunction. Other neurological diseases like ALS have been stated to include “misfolded proteins”. These are the proteins (enzymes) the body makes inside the cell and inside the mitochondria. ATP is a part of that process in both the mitochondria and in the cytosol – mitochondrial ATP is actually shuttled back to the cytosol for further chemical reactions. So if nutrients aren’t available, those chemical reactions can be interrupted and misfold the proteins they need to make or even fail to make them. Like getting interrupted when folding laundry and you misfold the shirt. If deficiency is corrected, those misfolded proteins can be corrected during subsequent cycling. If it is not, the problem gets repeated and dysfunction can become the norm. It can actually become “encoded” as DNA and RNA gets replicated during cell regeneration. When deficiency goes on for too long this further compromises the cell, especially if it is a nerve cell trying to rebuild its protective coating called the myelin sheath. It becomes the equivalent of trying to protect a window in a hurricane with cardboard instead of putting up wood panels, because the proteins are not made in the proper way, not strong enough to support functioning. They can then deteriorate and break quickly and cause cell destruction, known as apoptosis. This is how “degeneration” can start in the body.
Now let’s get back to Biotin and B12. Prolonged deficiency of Biotin, which can stem from undetected gene mutation preventing the body from efficiently recycling Biotin, is known to cause B12 deficiency. It will likely start out as functional deficiency of Adenosylcobalamin because the body can’t make MMA regularly needed to work with Adenosylcobalamin. The Methylcobalamin reactions of B12, the ones just before the Biotin reactions, can continue to function if all other related nutrients are in supply and help produce Propionic Acid and keep blood tests normal because the Methylation Process and Blood Cell creations function normally, so anemia will not present. (Pernicious or Megaloblastic Anemia will essentially Never present in this scenario and why doctors will never make a B12 connection based on how they have been trained. Macrocytosis will not present.) However, the neurological symptoms, skin issues and tingling and weakness and fatigue and toxin levels likely begin to elevate because ATP is not being formed and fatty acids, proteins, not being properly made.
This is because that main pathway, cycle, starts to break down. If a cell can’t complete the chemical reactions it can’t produce things the body needs. Hormones, gastric juices, saliva, mucous, pancreatic enzymes to break down food we need to get more vitamins, energy and oxygen for brain cells, the myelin sheath to protect nerves, even normal histamine reactions in response to allergens, and so on. Another irony is that the body likely can’t efficiently make the special proteins necessary to transport specific vitamins such as B12 to get into the cells – Intrinsic Factor, Haptocorrin and Transcobalamin production – three proteins critical to B12 transport – could be affected at this stage. Some B12 related issues have been stated to have deficiencies in these proteins but yet I have not found research making any note of the fact that they are produced in the body, so another process has to fail in order for them to be missing – can this then explain that deficiency? Biotinidase activity – the enzyme critical for Biotin recycling, may also be further compromised. Proper cell signaling cannot take place, ATP is a part of intercellular signaling, so the brain and glands and organs can miscommunicate and over-produce or under-produce critical hormones or other chemicals. It becomes a progressive state of deficiency and dysfunction. It is kind of like that old saying – “you can’t get a job because you need experience, but you can’t get experience if you can’t get a job”. You can’t get nutrients without nutrients needed to extract them – this is why our body is a “cycle”.
At this point we may end up taking different medications to deal with those individual symptoms, possibly making things worse. Many doctors may prescribe prednisone to stop the immune system and the miscommunication depending on the severity of symptoms. Sadly this can in turn lead to greater difficulties for the body trying to recover because it is still missing the raw base products (nutrients) to help it function normally. Proper nutrient replacement during that time frame would become critical in order to replace what the body was missing that caused the need for the medication – else you may not be able to wean off the drug without having the same reactions as before, or even more profound reactions.

Turning off cell functions, B12 and Biotin functions, may leave the body more vulnerable. This is the actual warning and side effect of prednisone and other steroids because the immune system is now nonexistent. Sometimes a body may have dormant viruses or protozoan infections that are being kept inactive and once the immune system is turned off they can cause havoc. (Examples are conditions like Shingles or Epstein Barr, in dogs Neosporosis) In some cases, new issues can arise from this steroid treatment. An example would be Exogenous (iatrogenic) Cushing’s, Cushing’s disease known to be caused from medication like prednisone or other steroids used to treat “allergy” conditions. This type of Cushing’s is usually Pituitary based – not necessarily a known tumor on the adrenal glands, though one could debate if this process caused a tumor on either the pituitary or adrenal gland. An interesting note is that Cushing’s cases in dogs are on the rise at a somewhat alarming rate – coinciding with an increase in allergy meds and prednisone use. There are also cases of steroid induced Diabetes, another condition on the rise in animals. Diabetes is actually known to be helped in some cases by Biotin supplementation since Biotin plays a part in glucose tolerance. I had a Cushing’s dog (the disease started after long term use of OTC allergy meds prescribed by her vet) that was helped by Biotin and B12 but I did not immediately make the connection at that time, else I could have been more consistent in supplementation of those in particular to abate her symptoms, but that is why I know what I know now. An additional piece of information is that in the case of Cushing’s disease, Cortisol, the “fight or flight” hormone overproduced in Cushing’s, is created in the body from cholesterol. This means that fatty acid metabolism is overstimulated to produce the hormone – further draining B12 and Biotin and creating even more symptoms. The reverse disease known as Addison’s, the underproduction of Cortisol, would be affected by the same deficiencies. Dysfunction and Miscommunication of the glands – which can happen from functions being “turned off” by steroids. Prednisone has MANY side effects but one in particular is of note – it usually increases appetite. With the body having its functions “turned off” – it is likely reacting by “thinking” it must consume more nutrients to fix the functions that have stopped.
Interrelationship of Vitamin B12, Androgens and Cortisol in Chronic Stress and Associated Vascular Dysfunction
Gut malabsorption begins to happen, maybe you get indigestion, you simply stop getting the nutrients you need to function, and the decline progresses. If you take an acid reducer or a PPI (Proton Pump Inhibitor), these are known to increase B12 deficiency because stomach acid is needed to extract protein bound B12 and Biotin from food along with other nutrients, so deficiency gets worse. The PPI can also interfere with Intrinsic Factor production in the stomach needed to transport B12. And ATP is how a cell respirates and removes toxins. So a body starts to increase in bad stuff. Cells can’t get rid of bad things, toxins– they can’t exchange CO2 and oxygen. (Succinyl-CoA – known as ATP – is needed to create heme which is the precursor to hemoglobin – the oxygen carrying protein. Iron uptake is connected to heme.) Cell reproduction, natural turnover, like red and white blood cells, or GI tract cells begin to break down, possibly leading to that famous leaky gut syndrome. If the body can’t efficiently reproduce red blood cells or platelets that is the first time you may see a regular blood panel start to show signs of general anemia – again NOT necessarily Pernicious/Megaloblastic Anemia that doctors are trained to connect to B12 deficiency. (Interestingly, Intrinsic Factor can play a role in Pernicious Anemia and why adult onset can be detected in a person’s 30’s or later) Iron levels, hemoglobin (a protein created by the body), at this time may also be affected so doctors can believe it is solely iron deficiency and provide infusions because they are not seeing the trained signs of B12 deficiency and would never suspect a supporting role from Biotin deficiency. And by that time, because of the natural turnover rate of blood cells, the body has been having serious problems functioning for at least 3 months, but likely MUCH longer. Liver or kidney function tests could begin to show toxin elevation, it is also possible that cholesterol levels rise at this point because fatty acid metabolism has begun to break down. Breathing problems, breathlessness, can also increase – panting in dogs even when they are at rest. (toxins build so the body is gasping for better oxygenation – this is known to occur with increased Propionic Acid levels) You may also notice heart issues, murmurs, dilated cardiomyopathy (“DCM”), as another metabolic product called Homocysteine elevates in early deficiency. Any heart problem “should” initiate a check of Homocysteine, but even that is not standard practice in veterinary or human medicine. Yet almost 100% of cases of DCM in human medicine is coupled with elevation in Homocysteine. If Homocysteine is tested and found to be extremely low, this would signify that methylation is already in an overall danger zone. Deficiency of B12/Folate/B6, one or more, is playing a huge role. Homocysteine is a toxin if it elevates, but it is a necessary metabolite in the body so low levels, just like high, signify a chemical functioning issue.
In some cases, if a body is already deficient enough to be having varied symptoms, even a cold or low level infection or from regular medication use, a drug or vaccine could send it over the proverbial edge. “Autoimmune” reactions, looking like the body is attacking itself, can really be the body failing to protect itself because of deficiency. This includes nerve degeneration because the body can’t properly make myelin. Autoimmune anemia is another way this can happen, especially if suddenly triggered after a medical procedure or medication or vaccine injection, even chemo. IMHA (immune mediated hemolytic anemia) is one reaction seen after surgical procedures or vaccine injection – Thrombocytopenia can be another. This can be the failure to produce red blood cells and platelets due to deficiency, or the production of inadequate cells because they are not able to replicate in proper fashion due to missing or misfolded chemical reactions. This can lead to spontaneous cell death known as apoptosis. (I did have a dog once develop fatal thrombocytopenia many months after having surgery and chemo for mammary cancer, but I did not know any of this back then) In some cases it could be assumed that there is undetectable internal bleeding causing the anemia. If severe enough a doctor/vet will start blood transfusions to try to patch the problem, which actually may transfer some additional nutrients from the original blood donor and help as the body tries to hold on. If it is indeed nutrient deficiency induced and supplementation not restored (like thru IV/Feeding Tube nutrition), the consequence would likely be terminal as the body cannot catch up. There is also a possibility of an actual known uncontrollable bleeding issue. In these cases a drug called Aminocaproic Acid (Amicar) is sometimes administered to control bleeding. This acid is a derivative (end product) of the essential amino acid Lysine in a metabolic pathway that requires Biotin to produce. It can then support the case that if Biotin is deficient in the body, the ability to control blood and bleeding issues naturally would be reduced. At this point, Biotin deficiency would also likely have caused severe B12 inactivity/deficiency compounding the inability to properly produce red blood cells and platelets. To take this one step further, this set of circumstances increases risk for stroke and aneurysm – already known factors of B12 deficiency.
Iron levels - Hemoglobin status - which is often looked at in anemia - has been shown to have a direct connection to Biotin
Biotin Deficiency Inhibits Heme Synthesis and Impairs Mitochondria in Human Lung Fibroblasts
https://academic.oup.com/jn/article/137/1/25/4664400
A brief NIH article explains the biotracing of some forms of Avidin. (The places they tend to congregate in the body) Though the experiment was done on mice, I found it interesting that one place is bone marrow, though other organs are targets including the spleen. That can mean that Avidin is able to remove Biotin from the very area that produces RBC, WBC, Platelets, T-Cells, Natural Killer Cells, Cancer Fighting Cells, Mast Cells and Stem Cells. Is this then the trigger of “immune” responses, anemias, leukemia, bleeding disorders, blood and general cancers, myeloma, lymphoma? Biotin and B12 are already known to affect DNA and RNA during cell replication. If cells are not able to complete chemical reactions due to deficiency, it is conceivable that this can be a trigger for adverse gene activity (activating recessive cancer or disease genes) or the ability to morph cells into a cancer state.
In regards to lymphoma – this small summary is about a study done with 3 different antineoplastic drugs (chemo agents) on lymphoma cells. The lymphoma cells were intentionally segregated into a Biotin deficient and Biotin supplemented category. The Biotin deficient lymphoma cells were found to alter themselves into a “survival mode” that prevented them from easily dying (perhaps why cancer is hard to eradicate in general). When these two groups of cells were exposed to the chemo drugs, the Biotin deficient cells could not be destroyed as easily. This would further extend to an explanation that Biotin deficiency in the body itself may alter reactions of normal cells causing “disease” – inflammation, cancer formation, unexplained changes in hormones or protein levels. Improper cell replication. If Biotin is then supplemented, the cells of the body can go back to regular functioning – perhaps the immune system can itself go back to eradicating invaders or abnormal cells. At the very least, if medication is needed to control some aspect, even a chemo introduced, it may also help a medication work better until such time as the body self corrects and the medication can be eliminated. Could this then be the explanation of why a chemo may work in some patients and not others? It could depend on their overal level of deficiency and nutrient intake. But knowing that some chemo treatments are meant to target the Biotin pathways means that it would have to be continually supplemented during treatment in order for it to work better. Biotin deficiency stimulates survival pathways in human lymphoma cells exposed to antineoplastic drugs https://pubmed.ncbi.nlm.nih.gov/15681168/
This study provides information on Biotin’s effect on gene expression and support of the immune system and inflammation response and its relation in the body’s Cytokine response. (cytokine response has been critical in recent Covid virus discussions) Biotin Supplementation Increases Expression of Genes Encoding Interferon-γ, Interleukin-1β, and 3-Methylcrotonyl-CoA Carboxylase, and Decreases Expression of the Gene Encoding Interleukin-4 in Human Peripheral Blood Mononuclear Cells https://academic.oup.com/jn/article/133/3/716/4688036 This is an updated link to the article. https://pubmed.ncbi.nlm.nih.gov/12612142/ This study explains how Biotin Deficiency increases the body's PRO-inflammatory Cytokine response - Biotin deficiency enhances the inflammatory response of human dendritic cells https://journals.physiology.org/doi/full/10.1152/ajpcell.00141.2016 Another interesting small study that concludes Biotin deficiency may indeed be more prominent than currently assumed. BIOTIN AFFECTS CYTOKINE METABOLISM https://portal.nifa.usda.gov/web/crisprojectpages/0207268-biotin-affects-cytokine-metabolism.html
Dogs have been KNOWN to get cancers in areas of injections. The idea then is to give a vaccine in a leg so that if a cancer tumor develops the limb can be removed and the whole body may not be affected. Dogs, like humans, can also be given nasal vaccines, sprayed into the nose area. Tumors in the nasal area are on the rise, coincidence? Dogs also are having an increase in neurological issues of the spinal column. Could a localized injection in that area rob Biotin triggering the inability of the area nerves or tissue to protect themselves? The other common issue with animals is the use of topical flea and tick medications applied directly to areas over the spinal column. Another trigger? That is on top of the fact that oral and topical flea and tick meds are themselves a form of neurotoxin targeting the insects. Avidin itself could be considered a natural neurotoxin since extended consumption will indeed affect the neurological system – this was even studied in ants. A localized injection containing it could then in theory debilitate tissue by crippling Biotin functions. If diet is deficient, like in the case of feeding whole raw eggs, uncooked or dehydrated foods that are ground together with whole raw egg or highly processed food that does not contain an adequate amount of Biotin, and gut bacteria not producing enough replacement or being compromised by antibiotics, decline can happen. In some cases quickly, in others it could take a few weeks or months as we notice symptoms progress because the body cannot catch up to deficiency. Many have theorized connection in neurological decline happening within 3-6 months from vaccinations – this can explain a connection.
If we go a step further in the human world – could certain injections cause the same type of reaction? I had a friend die of ALS. The one thing that sticks with me to this day is her repeatedly saying that “it all started after a dental procedure”. But the doctors said there was no connection. I don’t know the details of her testing or the progression of her symptoms – though I do believe it started as Bulbar ALS as it was affecting her jaw and speech first. But it now makes me wonder if Novocain and the use of Nitrous Oxide during her procedure, perhaps antibiotics afterward, coupled with a likely existing B12/Biotin deficiency due to years of cigarette smoking, lead to an undetectable decline. The inability of the area nerves to recover from the Novocain injection and the known inactivating, killing, of B12 by Nitrous Oxide. (please see the Nitrous Oxide section below for this Critical information)
I mentioned gut bacteria. We have all heard about how important the gut microbiome is to the health of the body. Our skin even has a microbiome, and, Propionic Acid is also located on skin. For animals their coat and proper fatty acid metabolism to keep it healthy is critical to their survival. Most people don’t understand the vitamins the microbiome can produce and how they can then go directly into the blood and lymph system to be carried throughout the body – including to the brain. One of those primary vitamins is Biotin and why doctors may believe you can’t be deficient because the gut makes it – but yet they know the gut can have issues and probiotics are a big industry. For a person or animal it is critical and under normal circumstances functions efficiently if not overwhelmed. Antibiotics can then cause a double whammy. They would not only be capable of killing bad bacteria, but that of good bacteria creating Biotin. If Avidin in the medication is playing a part at removing Biotin on top of it, the affects can be severe, and even deadly. I think of the issues in hospitals with C-Diff infection, especially in seniors. My dad had it after intestinal surgery and it added to his final decline as he was never able to leave rehab after his surgery. I knew about needing probiotics, but even those didn’t help. He also had TPN after that surgery and had to be on a ventilator for a short time. If I only knew then what I know now, about Biotin and B12.
Think of how often a baby or child is given antibiotics. Every little cold it seems the doctor will pump the system with them because we fear an infection getting out of hand. That is on top of the numerous vaccines they are bombarded with from birth – more now than at any other time in past decades. (Even adults and recommended/required vaccines) If the theory of Biotin robbing or simply the overloading on this metabolic pathway by vaccines and medications is indeed correct, there is no easy way to know if your child is deficient or is getting enough from food sources to rebuild their system. Nor to know if Biotin deficiency has already extensively undermined B12 in the body. But if we look at possible symptoms like rashes, dry skin, thin hair, pink eye, colic and digestion issues like IBS/IBD, gastroparesis issues, peristalsis issues meaning poor gut motility-constipation or diarrhea, urinary tract and bladder problems (poor bladder control is an early symptom of B12 deficiency, due to muscle weakness), hypotonia, developmental delay in walking or motor skills or learning disabilities, and yes, autism, we can relate the possibility. And then there is the feared symptom of seizures from extreme nervous system breakdown or the bottoming out from an “autoimmune response”. Children seem to be susceptible to never ending infections because the immune system is just too weak, perhaps because we are not recognizing what is making it weaker, as our vaccine protocol and antibiotic use has increased. Vaccines are including “multiple” types of vaccinations in one injection, meaning ALL of those different medications are competing to affect the antibody reaction coming from this ONE Metabolic Pathway. Common sense would appear to indicate that alone can affect the body. But since doctor appointments are a premium and time becomes a factor in meeting a schedule – they are combined and given all at once. This same progression of underlying symptoms can apply to our companion animals and even ourselves.
I mentioned autism and I know it is of great debate in relation to vaccines. We do know that vaccines do have many questionable ingredients and toxins, I am not negating that point. As I explained earlier, some of those questionable ingredients may actually be used because they act as “reagents” in the biotinylation process for the drug particles – they detach them from the Avidins. We also know it is still a case by case basis else every child would be effected, so other factors still control the outcome. However, if this theory of how deficiency starts is indeed correct, it would further support the work of an Australian Researcher, Dr. Gregory Russell-Jones. He created a website dedicated to his findings on autism that include specific nutrient deficiencies. The main deficiency being B12 and related nutrients needed to recycle B12 in the body, including B2 (Riboflavin). This could be the extension of how Biotin deficiency would create B12 deficiency, both functional and overall, leading to sensory, learning and motor function disabilities. He has also created and maintains a host of other websites dedicated to his findings on B12 related issues including Dementia/Alzheimer’s. (links provided at bottom of article)
A Biomedical Approach Via Telemedicine in the Treatment of a Child With Sensory Processing Disorder Using Diet and High-dose Biotin Intervention: A Case Report https://pubmed.ncbi.nlm.nih.gov/31043911/ A Case of Partial Biotinidase Deficiency Associated With Autism https://pubmed.ncbi.nlm.nih.gov/13680408/
I would also like to note that there have been many studies done that show smoking and alcohol use are known factors in Biotin and B12 deficiency – this also includes recreational drug use. It might be of interest to ALS patients that Lou Gherig was indeed a smoker in addition to his body’s high need for nutrients by being a premier athlete and propensity for athletic injury increasing nutrient need for recovery. Smoking not only requires the body to remove toxins from the lungs, in particular cyanide (for which B12 as hydroxycobalamin is the antidote), but it damages the saliva cells of the mouth interfering with Haptocorrin, and has been linked to Intrinsic Factor reduction in the stomach, two of the B12 related carrier proteins. Alcohol does the same directly to the liver by overloading its need to filter toxins and pass them on to the kidneys for excretion. The liver and kidneys depend highly on functioning B12 and Biotin. Toxin elimination in the body needs to function at peak efficiency and any overload will drain the body’s resources making it susceptible to disease progression. This can also be a connection to cancers and neurological and psychological issues in firefighters, other emergency service and military personnel, and even in high performance athletes. Any work that requires constant contact with chemicals and toxins – such as cleaners, hair dressers and certain construction personnel would also be at high risk. Having formerly worked in the World Trade Center, I am familiar with the ongoing deaths and PTSD issues with emergency and recovery workers and survivors and can’t help but wonder if this is the connection to this ongoing tragedy.
Injury to the body will also require nutrients to recover, which can put athletes in particular at risk. My relative who had Ampullary cancer actually had an injury to that exact spot of the body over a year prior to her diagnosis. The area was severely concussed on a fence. She was also a regular user of Ibuprofen, especially to deal with the pain from the injury, and did not take many additional supplements or multi vitamins that could have offset nutrient deficiencies, or the effect of the Ibuprofen. It has made me wonder if her tissue was prevented from proper recovery due to deficiency, leading to cell mutation/cancer.
Pregnancy is also a drain on resources in the mother – this includes after birth as milk production requires an increase in fatty acid metabolism – a function of B12 and Biotin. It may also explain the problem some mothers have in producing enough milk after birth as they can be too deficient in these nutrients based on diet choices. Animal studies have proven that increased supplementation of both B12 and Biotin has indeed increased milk production. A draining of B12 and Biotin to help a fetus grow can be the link to symptoms in the mother both during pregnancy and afterward, such as Postpartum Depression and Anxiety and even hair loss. It would also be a likely link to Gestational Diabetes. Everyone has heard about Folate during pregnancy – but it seems to be overlooked that B12 is a missing ingredient and Biotin would be just as critical. For those who have never seen the short documentary on B12 deficiency discussing this issue in addition to autism, blood clots, neurological and GI issues, it is linked at the bottom of this article. One should also take note that if a mother is deficient during pregnancy, it is possible to pass on deficiency to the child, making them more vulnerable to infection and other issues from birth – even to birth defects. Though Organic Acid testing and gene testing “may” be done at birth, it too may not reveal the tenuousness of the baby’s system in being borderline deficient, especially since the primary goal of testing is to note dominant issues and will likely not flag recessive/reduced functioning capacity. This could then put a baby at higher risk during vaccination. For anyone having trouble conceiving – direct connection to B12 deficiency has been made in studies – for both the mother and father. Discuss full testing and supplementation with your doctor if you are having issues.
I want to mention one more item in regard to “fatty acid metabolism”. Much has been hyped about Fish Oil / Krill Oil supplementation. This is in regard to studies that have shown “decreases” in beneficial fatty acids in the body in certain diseases. What if those decreases were simply caused by B12/Biotin deficiency not producing those acids in the body? During “allergy” and neurological symptoms for my dog, (I put that in quotes because I now believe her scratching was caused from nerve tingling due to deficiency), it was suggested to increase fish oil supplementation. I noticed that her neurological symptoms worsened during that time and then I researched the connection that started my knowledge journey. I have also noticed that same side effect in some humans I know and even in my own response to increased fish oil supplementation. Forcing the body to handle an increase in these fats could further drain limited resources of B12 and Biotin – making neurological issues worse. It can increase Methylcobalamin functions, raising Propionic Acid levels, overloading the body’s resources of Biotin, while decreasing Adenosylcobalamin functions in a borderline deficient body – increasing neurological symptoms. Unbalancing the acids in the body and increasing their negative effects. If you have noticed the same issue in yourself or a loved one this could be of significance to you.
Modern day diets should also be taken into account when deducing the chance of dietary deficiency contributing to issues. B12 comes from meat, seafood, eggs and dairy – the highest source being liver. The highest sources of Biotin come from yeast, liver, soy and eggs, along with nuts and peanuts. Though for Biotin there are indeed other sources, just at much lower levels of concentration. A “liver cocktail” is actually what was discovered to “cure” B12 deficiency many decades ago. That cocktail not only included the natural forms of B12, but it included Biotin and a host of other B vitamins and minerals, therefore overriding any related deficiencies. If you look at the other items I listed above – they are often considered “allergens” in today’s world. Peanuts, for which peanut butter sandwiches used to be a staple in many children’s diets when they would go to school, are now banned in most schools so consumption of that critical Biotin source would also be reduced. So if they are intentionally avoided, the body can naturally become deficient, especially a growing body and brain in need of nutrients for proper growth. This includes Gluten because traditional flour products are often enriched with B vitamins – including Folic Acid – because it was determined this could lead to birth defects so enrichment helped to supply nutrients in a food source that people usually consumed. Avoiding gluten means to avoid breads with yeast – a high Biotin source. Avoiding meat and dairy also reduces availability of natural Biotin and B12, especially in the form of Adenosylcobalamin, in addition to other vitamins. People who have seen “positive” effects from going vegetarian or vegan – are actually reducing their intake of specific proteins, like Methionine, that require B12 and Biotin to metabolize. By reducing specific proteins they reduce the “load” on the body and give it an opportunity to “catch up” with underlying deficiency, preventing it from needing to convert Adenosylcobalamin back into Methylcobalamin to support methylation. One of the first course of actions for a body in a state of Propionic (PA) and Methylmalonic (MMA) Acidemia is to reduce protein intake – specific proteins of Valine, Methionine, Isoleucine and Threonine – allowing the body to catch up with any deficiency and balance out acid buildup – perhaps offsetting low functioning Biotin (partial biotinidase deficiency) that may not be genetically recognized. Though it can sound then like this is the cure for all disease, it is not. In a normal body, we will eventually need to get back to intake of the missing elements to keep up with demand for replenishment from exercise and increased daily functions and the ability to rebuild muscle and tissue – the body may also need more if any medication is effecting nutrient issues. The instance of disease and cancer in vegetarians and vegans is not necessarily any different than that of other diets. Moderation is of course the key to balancing a body. But since we are indeed genetically different, any one person can choose to debate the pros and cons of certain diets. I am simply giving information on how diet can effect deficiency and not taking a stand on diet or lifestyle choice. Of course, there are medical reasons and necessities for avoiding certain foods, and those who feel better on certain diets may be instinctively avoiding things that THEIR body cannot properly handle due to genetic mutations. Any one person should just keep nutrients in mind when examining if a diet could indeed be deficient in certain elements. (One special note for anyone who has been using protein supplements trying to rebuild muscle or put on weight. Check your ingredients. Some supplements, even protein bars, can contain Egg White. It can be dehydrated or freeze dried and ground into a powder. As explained earlier, even pasteurization of egg white does not deactivate Avidin. Some “natural” protein bars – usually refrigerated versions that are not baked (baking will deactivate Avidin)- can contain Egg White as a binder. If you have neurological issues you should stop using these immediately. This would also pertain to any whole raw egg added to smoothies or feeding tube formulations or dried egg white or whole egg powder.)
In a separate section below I also describe in detail another concern in modern diets – this is about Glyphosate and other herbicides and their effects on the body. In general we are unaware at how much Glyphosate can be consumed from our diet since it is used liberally in grain and vegetable farming. Even to dessicate grains at harvest. Glyphosate actually can have a direct connection to Biotin and other nutrient deficiency in the body and I explain how it can cause the problem. Please read that section to understand its unrecognized role in both humans and animals.
Biotin deficiency, in turn leading to B12 deficiency, as I have laid out with the details and scientific reasoning, can ALL happen without detection. No simple blood panel will ever show the early signs – this includes why even a Serum B12 test can be misinterpreted. That infamous saying “the blood tests look perfect”, but yet the symptoms are increasing and the doctor is perplexed. Each symptom can get treated individually without anyone understanding it can be related, or be a precursor to a more sinister disease progression. It can also be “assumed” by the doctor that it is “all in your head” since the blood work doesn’t show anything but yet you know something just isn’t right. It can easily explain why neurodegeneration, like ALS or DM in dogs, can be so difficult to diagnose – essentially a conclusion based upon elimination of other things. And why it can progress quickly or slowly, maybe even get “cured” (as more of the nutrients are consumed), and no one knows the underlying cause. Doctors have made assumptions that symptoms “cannot” be related to certain nutrients or even certain nutrient levels, without understanding why or how those levels can be compromised in the first place, or that they can even be misleading and hiding a deeper deficiency. The body has a natural cycle of cell regeneration from blood cells to organ cells, so if deficiency isn’t caught and supplemented early, dysfunctional cell replication can begin to get out of hand. Neurodegeneration will progress and no one will be the wiser. If your doctor has ever commented that if you eat meat, fish, eggs or dairy that you can’t be B12 deficient – THEY ARE WRONG. You can be Functionally B12 deficient and/or Biotin deficient and Every Doctor Can Misdiagnose It. By the time any standard blood test “might” show an indication of deficiency (anemia signs) – a body can already be in final decline and may not be able to recover. But as a reminder, if B12 is supplemented alone, anemia may NEVER present, B12 levels will remain deceivingly elevated, but yet neurological deterioration will continue. (The B12 video at the bottom of this article contains the case of a Medical Doctor who himself was dying of B12 deficiency before a blood test finally showed the severe progression)
Earlier I mentioned how medications can disrupt the Biotin pathway and be overlooked. I also mentioned that there are medications that are KNOWN causes of B12 deficiency. A scientific paper dated 2016, co-written by experts in B12 from Germany, Norway and USA, makes note of one such medication – and it actually supports my statement in this article on Biotin. However, the experts do not even appear to realize the possibility of this issue. In the paper they make note of Metformin – a very widely used Diabetes drug. The paper notes that use of Metformin reduces Serum B12 and even Haptocorrin, however, it also reduced MMA levels, and they noted increased intracellular activity of B12. In the scenario I have laid out – this fits perfectly. Metformin could affect Biotin, that alone decreases MMA. Decreasing MMA will increase intracellular B12 activity because ATP cannot be formed with Adenosylcobalamin – meaning cycles are getting interrupted. As Mitochondrial function decreases from this, Methylation increases trying to support functionality and likely converting Adenosylcobalamin from the Mitochondria into Methylcobalamin in the Cytosol – therefore appearing as an increase in intracellular B12 activity between the Mitochondria and Cytosol. The body “may” be interpreting the missing ATP and subsequent missing chemical reactions (like not creating Haptocorrin) as a trigger to increase methylation to stimulate functions – trying to increase the “cycle”. Serum B12 levels eventually drop as the body speeds methylation, burning B12, in an attempt to compensate. So Biotin deficiency, interference of the Biotin pathways, is causing B12 deficiency and the reduction in MMA. (Metformin may use or effect the SMVT protein – sodium dependent multivitamin transporter – which is utilized by Biotin, B5-Pantothenic Acid, and Alpha Lipoic Acid and is a link to the nutrients crossing the Blood Brain Barrier) This would further support the information on B2 deficiency from Dr. Gregory Russell-Jones since the body would then “burn” more B2 trying to recycle B12 to increase methylation. As both levels of deficiency rise this can then lead to muscle/tissue wasting as the body attempts to gain more nutrients by using its own resources to function, even trying to increase ATP from other metabolic pathways. The levels in particular that may show this phenomenon would be Propionic Acid and related Biotin markers. From a neurological standpoint, this would “mask” the signs of B12 deficiency causing neurological issues because “early” testing would likely reveal normal / high normal Serum B12, MMA would test at normal or low normal levels (at the very least, levels “in range” because Biotin was not functioning efficiently), and Homocysteine may also test at normal levels because methylation is continuing until such time as B12 becomes too low from overstimulation. Only then would methylation begin to slow or fail and signs of anemia present. This can be the link to diabetic neuropathy – for which another medication may be prescribed to prevent the pain, in turn making depletion worse. Once again, if B12 is supplemented, it would likely continue to support methylation and possibly raise Serum levels, but neurological decline would continue unless Biotin is supplemented.
The paper in which the Metformin information appears is titled: Biomarkers and Algorithms for the Diagnosis of Vitamin B12 Deficiency https://www.frontiersin.org/articles/10.3389/fmolb.2016.00027/full
What can fix this? Do no harm. If Biotin robbing, or even pathway corruption, is the actual consequence in the case of Vaccines and Medications, then in theory it may be possible to replenish what is robbed as Avidin leaves the body or recycling gets overloaded. Bioengineers may be able to replenish Biotin in the same medication or vaccine. Since Avidin is already bound to the biotinylated nanoparticles, free Biotin could be included in the mixture to be available to rebind when the nanoparticles detach. That would mean they could at the very least replenish what the medication would be removing. Ideally, providing amounts above that figure may be more prudent to make certain we do no harm and leave the body in a hopefully better state. Knowing calculations of how much of a drug is being administered via Avidin binding means they would know how much free Biotin could be bound and removed from the body. That would allow them to match that amount to make certain it stays the same. Is this practical? I admit I am not certain since this is a cellular reaction and the guarantee of free Biotin being available to that particular cell or area of the body may still be of issue – genetic biotinidase insufficiency could also play a part in cellular failure. But if enough is in circulation in the body, it may prevent adverse reactions or long term side effects from use, the same as it would for people who do not get an adverse reaction. Would this inhibit absorption of the beneficial drug before it would be excreted from the body? Again – I do not know. Since many medications are metabolized in the liver, the highest concentration point for Biotin and B12, it could indeed protect the body by keeping the liver healthy. Admittedly there is also a chance it could be counterproductive to any particular lifesaving medication such as an antibiotic. Antibiotics are meant to kill a bad living organism in the system that may itself use Biotin to replicate. Some specific strains of intestinal yeast infections are known to thrive with Biotin supplementation. However, understanding why an adverse reaction could happen from the medication, and how to counteract with Biotin supplementation, would be helpful for patients and doctors. After the infection clears, a course of supplementation could resupply and rebuild the immune system. Most of us do this with probiotics because we know we need to replenish good bacteria. Knowing Biotin could be a key allows us to replenish that alone to help critical metabolism functions. A full B-Complex and quality multivitamin at the very least, may be more prudent to complete nutrient cycling and make certain of adequate intake of all related chemical catalysts.
I wrote this article intentionally to combine both human and animal cases. I tried to use as simple but yet complete a basic scientific explanation as possible to convey the very complex and technical processes and reactions the body goes through. Since my focus was to describe how Medications and Vaccines can directly effect deficiency and disease, I also limited further technical information on B12 and Biotin in the body – but have included links to studies at the bottom. My goal was to help people think about the symptoms they are seeing in both humans and animals in order to connect their own dots. Does this apply to 100% of cases? Likely not – but then we know not every person or every animal will react the same way to any one drug, vaccine or treatment, and yes, genes can still play a HUGE part in making any patient more vulnerable to deficiency and disease progression – like the reduced ability to recycle Biotin due to genetic mutation. A gene trigger may simply be the level of deficiency in the body – even if it is slight. An overload on one metabolic pathway that is being exploited by a myriad medications and vaccines. If we keep beating up one metabolic pathway for everything, it really is common sense that it may be buckling under the weight and leading to system (body) failure.
Doctors and veterinarians are so overwhelmed these days that they can’t immediately recognize a connection between ongoing or progressing symptoms or possible risks in their patients. How each new symptom, even being caused by a new medication, could be linked back to a main cause, a deficiency, instead of thinking it a new disease to treat. A progression of deficiency happening in the body that is triggering new symptoms, which can be different from patient to patient. GI symptoms progressing to Allergy or Heart Issues or to Diabetes, to Cushings, to walking issues, neurological decline, etc etc. Maybe thinking twice before they prescribe a steroid or allergy medication. Medical professionals in most cases need to treat symptoms for expediency – hence the use (overuse) of steroids. We have learned that we have to be our own advocates, for ourselves, our children, and our pets. And I can tell you from personal experience that if you even try to mention B12 or Biotin to a doctor or veterinarian as a possible cause or to assist in symptoms, you might as well just talk to the wall because they will dismiss you and think you crazy, unless they happen to understand nutrients. They typically don’t think of either as medicine when they most definitely should – especially in cases of acidosis. And drug companies might have a pill for that, so they just prescribe it. But as that old saying goes, Food IS Medicine. Vitamins and Minerals are what the body uses to work in chemical reactions. If they are missing, the reactions fail. Plain and simple.
The article on Avidin that I referenced earlier, that was first published in 2016 – The Principles and Applications of Avidin-Based Nanoparticles in Drug Delivery and Diagnosis, has a particular sentence in the last paragraph of its Conclusion section that I thought poignant to quote in the context of this writing:
“Despite of multiple advantages of this system in biotechnology, further research is required to understand the immuno-toxicity of the avidin and its variants.”
That line alone can support the theory I have proposed, that this delivery system, and its overload on the Biotin pathways, can indeed be creating an issue that No One Is Recognizing.
In the following sections I break down additional details that most do not know – including medical professionals. I explain why Nitrous Oxide is dangerous and how problems may not show up until months after use during a medical procedure – evading any connection to that original cause. I explain various specific testing that can be done to identify Biotin and B12 issues. I also explain certain treatment options. I include a section on why there is an FDA Warning about Biotin use – it has NOTHING to do with ingesting Biotin but rather its connection to the bio-engineering of common testing procedures. Biotin use can skew test results including tumor marker tests and hormone and enzyme tests leading to misdiagnosis. This is not common knowledge among doctors doing blood work.
The sections below are:
Nitrous Oxide Warning
Treatment
Testing
Vitamin Recycling and Muscle Wasting
FDA WARNING
The Glyphosate Connection (Roundup and other Herbicides)
Pet Owners
______________________________________________________________________
Nitrous Oxide Warning
Special note for anyone with neurological issues following the use (or possibly unknown use) of Nitrous Oxide for dental or medical procedures – even within weeks to many months after a procedure – even up to one year. Nitrous Oxide irreversibly inactivates B12, a medical scientific fact. It chemically kills its action in the body. The longer it is used for a procedure, the more damage to B12 is done. If a body is very deficient before a procedure utilizing Nitrous Oxide it could cause an extreme downfall collapse within a short time frame from a procedure, days or even a week, month or even many months more as the chemical reactions begin to fail from deficiency. Nitrous Oxide is thought to be safe and stated to have a better “analgesic” (pain relieving) effect on the body during recovery. Sadly this “positive” response is likely because it kills B12 reactions thereby disrupting the ability to send pain signaling. That “killing” effect may however not show up on any standard B12 test because a standard Serum B12 blood test CANNOT differentiate between active usable B12 and that which is UNusable for the body. (a fact doctors do not always understand) If coupled with Biotin robbing/disruption from Novocain or another nerve block or other drug used during procedures, even antibiotics after a procedure to prevent infection, this could potentially lead to the start of neuronal breakdown such as in ALS and other motor neuron diseases and would all go undetected in standard blood work. An extreme anemia event or neurological collapse would also be possible within a short time frame from a procedure if the body was seriously deficient beforehand and not enough nutrient replacement instituted afterward. The one test that may show immediate indication of B12 damage could be MMA if Biotin is still functioning and producing adequate amounts. For anemia, Homocysteine “should” indicate an issue. However, if MMA levels fall “within range”, they too could be misinterpreted. If Biotin is deficient and a contributing factor, MMA levels could still be lower and not cause concern. Biotin markers, in both blood and urine, (such as propionic acid levels, beta-hydroxyisovaleric acid, biocytin) should be tested at the same time as ALL forms of B12 (Serum B12, Urine MMA and Serum MMA and Homocysteine). This would give a more complete picture as to B12 status – inactive, versus overall deficient, and if Biotin deficiency is playing a part in the system “collapse”. The reason to test both urine and serum is to establish how much the kidneys may be filtering to offset dangerous levels in the blood. If both are in the “high or high normal” range, coupled with neurological symptoms, it can indicate that B12 functions are not properly completing and the body is trying to balance the toxin levels. Any elevated or “normal” B12 level on a serum test would then be showing inactive B12 masking the issues. If Biotin is still functioning properly (usually indicating high MMA), there are other nutrient deficiencies that can inactivate full B12 cycling and deceivingly elevate serum B12 levels. These can include deficiency of B2, Iodine, Selenium and/or Molybdenum, leading to a misunderstanding that B12 is not effected based upon Serum levels. Making it more important to test MMA. Those deficiencies would prevent the ability of B12 to recycle. (explained further below).
I found the following article, written in 2018 by a trained dental anesthesiologist, very enlightening. It appears, even though the dangers of Nitrous Oxide to B12 have been known for a very long time, it STILL IS NOT common knowledge in the medical/dental profession. The Link between Nitrous Oxide Uptake and Vitamin B12 Deficiency https://www.todaysrdh.com/the-link-between-nitrous-oxide-uptake-and-vitamin-b12-deficiency/
The problem with Nitrous Oxide exposure, and why it is often not thought to be connected as a cause of neurological or hematological issues unless a patient is known to abuse whippets, is because it can be a delayed reaction – by weeks or even months. Once B12 is “killed” it takes time for a cumulative negative effect to build in the body – all dependent on the state of B12 in the body and if a patient ingests regular B12 supplementation and supporting nutrients (outside of just diet choices) to offset reactions and aid the body in recovery. As cells try to replicate and repair, if a deficiency exists in the body and more B12 can’t be sent to the cells, cell replication and chemical reactions (like producing myelin) begin to fail and take time to affect the overall system. The body can even convert B12 from Adenosylcobalamin into Methylcobalamin to keep Methylation functioning – blood cell creation, toxin removal and other critical aspects of methylation. Red blood cell turnover rate in the body is approximately 120 days – meaning it can take at least that long to start to see hematologic signs of anemia from deficiency – 3 months or longer. The draining of Adenosylcobalamin will begin to affect the neurological pathways but blood levels of B12 will NOT show the severe affects. Even homocysteine as a marker may not yet show elevation because methylation continues. Anemia will not be a symptom, but the neurological symptoms will likely increase as time progresses unless supplementation is started. If only mild supplementation is started (such as oral instead of injection, especially as just methylcobalamin), neurological decline can still continue since oral is limited through absorption and anything that is absorbed will likely go to support methylation functions and may not convert into Adenosylcobalamin. Oral supplementation will also affect Serum levels, giving a false sense of security by raising circulating Serum B12. However, MMA can increase during this time if it is properly checked and Biotin is still functioning. This is why doctors and dentists often dismiss any connection to a dental or medical procedure – because they simply do not understand how the body can be getting worse that far removed from the procedure date. This can be a Deadly Misunderstanding.
This same scenario also exists for animals. Some veterinarians use Nitrous Oxide mixed with Oxygen as part of their procedure when they aerosolize certain anesthesia medications when placing a mask on the animals. Some veterinary texts and articles have touted its use as a “safe” method without any note of the effects on B12.
The use of Nitrous Oxide during any procedure is often NOT considered part of the anesthesia “protocol”, except maybe for a dentist. If you enquire about what drugs were used during a procedure you will likely get a response like Propofol or Fentanyl. Nitrous is a gas and therefore not a prescribed drug. For both human and animal procedures you must ask explicitly if Nitrous Oxide is used with Oxygen during a procedure. This may only be known in human cases if asked directly to the anesthesiologist as written records for anesthesia may not reveal this nuance.
Again – please keep in mind that the use of Nitrous Oxide and Novocain (or any other type of nerve blocking agents) together “could” potentially affect nerve recovery by effecting B12 and Biotin. For any progressing neurological symptoms after a procedure, complete testing would be the only way to know, and complete supplementation may be the only way to reverse symptoms. If complete testing cannot be done – starting a course of Hydroxycobalamin injections, no less than one per week depending on severity of symptoms (possible daily in severe cases) as soon as possible, would do no harm to a body (no overdose possible of B12) and provide the safest method to attempt the halting of neurological decline. Providing increased Biotin intake at the same time would also make certain it is available in the body for activation of Adenosylcobalamin once the body begins to rebuild its supply. Biotin also has no concern of overdose related to use under normal functions and actually has a naturally short half-life and will be excreted if not utilized. A complete B-Complex and/or Multi Vitamin would additionally be helpful to assure availability of any additional missing nutrients including those necessary for B12 cycling. (direct concurrent Adenosylcobalamin supplementation may help the body correct quicker if there is any issue with conversion into this form)
A German nutritional researcher, Dr. Bodo Kuklinski, who has done extensive studies and writings on Mitochondrial and Neurological issues, has expressed that high dose B12 supplementation should always be done in concert with Biotin supplementation. He has stated neurological improvement may not be recognized in many cases and skin issues can increase as B12 supplementation increases chemical reactions in the body and drains Biotin. If Biotin recycling is an unknown factor (biotinidase issue), supplementation would obviously improve chances of recovery making certain free Biotin is in circulation. Please understand that this all should be done in direct consultation and guidance of your doctor(s).
There are many articles that refer to Folate (aka Folic Acid) “masking” B12 deficiency. Some dentists have even misinterpreted Nitrous Oxide issues to mean that it effects Folate and not B12. Folate works with B12 in the Methylation cycle – an extremely critical function in keeping blood cells flowing, replicating and transporting nutrients and toxins. Deficiency of either B12, Folate or B6 is known to affect methylation, raise homocysteine and cause anemia. So if the body still has an adequate supply of Folate and B6 it will continue to keep Methylation going by combining with B12 as Methylcobalamin – even if the body needs to convert from Adenosylcobalamin. Methylation functions need to happen to keep organs functioning. When Methylation breaks down, THIS is when the signs of anemia will begin to show on a standard blood panel. If a doctor does not pay attention to the neurological signs, it will progress to this stage and could become a severe situation quickly. If blood tests also reveal a Folate deficiency – it can be because B12 is already deficient enough that methylation has slowed and therefore the body simply excretes unused Folate. Folate, in most cases, should not be supplemented without supplementing B12 at the same time. Remember, a B12 serum test could be inaccurate and showing levels of “inactive” B12. Increasing Folate could cause B12 to further drop and increase neurological symptoms. It is known that in most cases supplementation of Folate alone will not improve neurological symptoms – leading one to deduce that the B12 level, if taken and appearing normal, could be inaccurate. In the case of Nitrous Oxide – the B12 level could be reflecting chemically unusable B12. At this point, another medication or vaccine or procedure could cause a cataclysmic downfall that no one may understand.
I am going to add a personal hypothesis regarding Nitrous Oxide and Medication use. Teens and children appear to be having increased psychological issues. Dental procedures for wisdom teeth removal and even installation of braces, or for fearful children in dental offices, may include use of Nitrous Oxide, as noted in that above linked article, just as it did for me as a teen. Add to that the possibility of repetitive antibiotic use for colds and flu, even for a dental procedure. The possibility of high stress in children and teens in social issues or in athletes, high achievers, family issues, etc., and it could create the perfect storm for severe deficiency. This can then lead to a higher risk of injury for some athletes, continual colds or infections, problems with thinking and school work as deficiency can effect brain function, and even psychological issues related to deficiency, possibly leading to “acting out” or mood changes. I personally can attest that I had issues in my youth and I came from a family of smokers, I had an ulcer as a child and was on acid reducers, and I had Nitrous Oxide for wisdom teeth extraction that was apparently more complicated and longer than usual and I had trouble waking up from the anesthesia. I seemed to have more “trouble” functioning in class, especially after that time, and now I can only wonder if that was the cause. School nurses may not be versed in the possible side effects of Nitrous Oxide used for procedures and would not know to warn parents to the possibility. School nurses likely also don’t understand the depths of B12 deficiency in general. If even doctors don’t believe it a possibility in adults, children and deficiency would never be on their radar. Since even cases of ALS and other motor neuron diseases are now being reported in teens and young children, not to mention learning disability issues, could this be the start? Coupled with endless medications and vaccines, including diagnosis for ADHD and other disorders and Autism. For the sake of mental and physical health in children, avoiding suicidal tendencies – B12 deficiency, both functional and overall deficiency, should be a consideration, and Biotin deficiency caused from medications and vaccines, even diet deficiencies, should also be considered. (Parents should also consider asking their pediatrician/OB-GYN for any copies of Organic Acid testing and Gene testing done at birth. It may reveal recessive gene mutations that can stipulate less than optimal functioning in critical areas, such as Biotinidase or Mutase, which could potentially lead to issues. If Biotinidase is suggested to fall under 50% optimal functioning you may want to discuss long term supplementation to ensure that no medication or vaccine creates an issue.)
___________________________________________________________________________
Treatment
Please understand that correction of all issues, especially advanced neurological issues, may not mean simply supplementing with small amounts of Biotin or B12. Depending on the length of time and advancement of deterioration, can also mean complete reversal may not be feasible, though dramatic improvement in symptoms within a year or more may indeed be possible with continuous treatment. If advanced B12 deficiency does exist as a result, it likely would not mean a simple B12 supplement either, though BOTH Biotin and B12 should be resupplied at the same time to make certain cycles can function and any general gene abnormality will not inhibit reactions. Severe B12 deficiency must usually be treated by injection, likely daily or every other day injection of Hydroxycobalamin, to make certain a supply is circulating in the body. Severe deficiency of B12 can also mean that the body may be better served by additional direct supplementation of the Bio-Active forms – Methylcobalamin AND Adenosylcobalamin (aka Dibencozide) – to make certain deficiency or gene mutation does not prevent conversion issues from one form to another and recycling issues from corresponding deficiencies. Care however must be taken to address potential adrenaline reactions that can be associated with Methylcobalamin in particular.
As a gauge, I wanted to describe what some have used as dosages for Biotin in the face of neurological and diagnosed conditions. In Biotinidase deficient/low functioning children and adults, I have been told that some have success using low dosing (1-2mg per dose at 2-3x per day) to help quell symptoms. In other cases, some adults have used 5-10mg per dose at the 2-3x per day range. MS patients have been using 100mg in dosing at 2-3x per day. (The MD1003 study involved 100-300mg per day and it has been successful for many MS patients – patients it did not work for may have been missing related nutrients such as adequate B12 to complete cycles, but this was not tested) Biotin has a half life that can mean it burns off quickly in the body or gets excreted before use. Dividing dosing throughout the day allows for it to stay in the system and be utilized when needed, especially if other stresses in the body require more reactions. High Biotin use MUST be taken into account for ANY BLOOD TEST. PLEASE READ the FDA WARNING section below to understand why and how Biotin can cause adverse blood test results so you must abstain before testing – it can lead to inaccurate diagnosing if it alters a blood test. This information is meant as a guidance ONLY and you should discuss any supplementation protocol with your doctor to understand if it is right to try for your situation.
Some papers, and experts, have stated that a supply of all three forms of B12 (Hydroxycobalamin, Methycobalamin and Adenosylcobalamin) may best help replenishment for a severely depleted system by ensuring the body can restart dormant functions without the issue of converting any one form. Some neurologists have seen positive results with use of Adenosylcobalamin alone or in concert with Hydroxycobalamin injections. Related supporting nutrients to keep the body functioning, such as B2 for B12 cycling and all related B vitamins (they work together) must be kept in constant supply – this includes Biotin. Related nutrient interactions coming from Selenium, Iodine and Molybdenum must also be a constant supply in order to convert B2 to its active forms of FAD and FMN for the body. (Please refer to the research and guidance of Dr. Gregory Russell-Jones from his linked websites to understand these and other nutrients.) If you feel this could benefit you or a loved one please discuss all supplementation choices with your doctor(s).
It seems in many countries, B12 deficient and diagnosed Pernicious Anemia patients are having trouble getting prescribed injections. Oral supplementation effectiveness has been disputed by many researchers – though this was never narrowed to see if it effected certain forms of B12 (synthetic cyano versus methyl versus hydroxy versus adenosyl). Much may have to do with other unrecognized deficiencies, such as Biotin, preventing proper conversion and utilization of oral supplements. More studies would need to be done in this area to see if that is indeed the case. I felt it prudent to mention that some B12 supplementation in the form of Methylcobalamin, often combined with synthetic Folic Acid as its methyl exchange partner, can be obtained with the gut absorption protein called Intrinsic Factor. (pernicious anemia patients may actually have trouble making this protein – again, possibly due to biotin deficiency) A US company called WonderLabs has made a B12 product (Trinfac-B) used by both people and dogs (dogs with EPI), with great success because it contains a favorable amount of Intrinsic Factor allowing for GI absorption. There are also a few brands of B Complex available that include a nominal amount of Intrinsic Factor for this very same reason. Douglas Laboratories is one distributor. A search of Intrinsic Factor in popular retailers should yield results in this area. Again – this is for information purposes ONLY.
Though supplementation can resupply what is being effected by medication, it could also affect how medication may work and thereby fight one another. In some cases, medication adjustment (titrating dosages) might have to be made as the body replaces lost nutrients that could have caused the need for medication. This can be critical for certain long term medications and doctor guidance becomes Highly important, especially with seizure drugs, heart or diabetes medication. A doctor who is well versed in nutrients (such as a Functional Medicine or Naturopath or Advanced Nutritionist) can work with you to plan out a supplementation course that should take any medication into account and rebuild the body slowly with enough nutrients to restart chemical reactions and increase them as the body may get stronger and in turn prevent an overdose or interaction of any one nutrient. Please understand that if deficiency is the underlying cause, restarting chemical reactions can sometimes strain the body and cause additional symptoms. B12 and other vitamin replenishment may also require certain nutrients to be in the diet in adequate amount, such as potassium, by increasing potassium rich foods daily, to quell adrenaline reactions such as heart palpitations or shortness of breath, known to happen with supplementation and severe deficiency. These reactions happen because dormant chemical reactions, like those misfolded proteins, can be restarting in the body. These can be scary when not understood. However, with some medications, increasing potassium can also be a concern since the medications can cause a body to retain more potassium – check the drug labels. This is the “catch 22” in supplementation versus medication. CONSULT YOUR DOCTOR.
If you are taking any medication, especially those for pain, simply because of the reasoning I have laid out with Biotin robbing and interference, it can be an uphill battle to fix what is wrong in the body. Pain medication is designed to STOP nerve signaling. If you are trying to FIX nerves, pain meds can further complicate the issue. If you are taking meds to control Diabetes or Heart problems or Seizures – all known to affect B12, likely via Biotin interference, it can be a hard situation to resolve without close attention to how the medication will be effected by supplementation. And stopping anything abruptly after a body has been kept in a balanced state can cause serious harm so it MUST be done with MEDICAL GUIDANCE.
To reiterate – Genes can play a part in why the body began downfall and how it adapts when supplementation starts. There are many genes associated with B12 function and even Biotin function. This can affect the type of supplementation the body responds well to, including types of Folate (synthetic Folic acid versus natural Folinic Acid or Methylated Folate) – those with a gene mutation MTHFR would be familiar with this response. Methylcobalamin may also cause agitation as the body ramps up methylation functions and therefore only Hydroxocobalamin or Adenosylcobalamin (aka Dibencozide) may provide a safer relief of symptoms as the system rebuilds. Doctors trained in these nutrient reaction areas may better guide supplementation choices to alleviate symptoms.
In terms of particular B12 related genes (see the Testing Section), it is remotely possible that an increase in Biotin can trigger a worsening of symptoms. The reason is because Biotin can increase MMA. If a body has certain gene mutations involved with the conversion of B12 to Adenosylcobalamin, and direct Adenosylcobalamin is Not supplemented to bypass the anomoly, MMA can build without the ability to be consistently converted with the help of Adenosylcobalamin. MMA then becomes a dangerous toxin. Though this is likely a rare instance, it is possible. It would likely have been known early in childhood development. But since it is possible, I wanted to alert anyone to the possibility of an adverse effect from increasing Biotin. It may mean that direct Adenosylcobalamin supplementation can offset reactions, and may actually be the primary solution to alleviating symptoms.
Many who have neurological decline – especially ALS – have tried various supplementation to aid the related symptoms and trying to halt progression. Many of those supplements can be considered “End Products” of Metabolism. What that means is, if certain nutrients (vitamins and minerals) and chemical reactions were already properly functioning in the body, those very “end products” would be created normally by the body. This includes certain enzymes that many take as a supplement.
One supplement is SAMe which works within the Methylation cycle of the body and requires functioning Methylcobalamin to naturally produce. If you start supplementing B12, especially as methylcobalamin, and even take additional Folate – taking SAMe can actually be counterproductive and cause additional symptoms/issues. It may cause jitters and irritability.
CoQ10 is another supplement that the body would produce with adequate levels of B12. CoQ10 is known to deplete with age (as does B12) or with certain statin medications. The statins are actually directed at the Biotin/B12 pathway which is likely why CoQ10 is being effected. However, unlike SAMe, there does not appear to be a problem with supplementing additional CoQ10.
Other items work to improve the functioning of Methionine/Cysteine in the body – critical to Methylation and a precursor to Glutathione. Even Melatonin is an end product that requires B12 to produce naturally. Taking additional Melatonin to aid sleep and gut function can be helpful as the body rebuilds B12, but should not be necessary long term if B12 and Biotin is replenished.
Another called NAC (N-acetylcysteine) is being tried by some patients to help with mucous, inflammation and lung function. This drug/supplement was originally invented as an antidote to counteract liver toxicity from acetaminophen overdose and recently has been used by Cystic Fibrosis, COPD and HIV patients to help with lung function. It is designed to increase cysteine functions and is considered a precursor to glutathione. When the body has B12 functioning optimally, metabolism of cysteine and methionine works efficiently. It is part of the critical “Methylation” system in the body that starts the Propionic Acid process. Methionine requires B12 to metabolize. In a state of deficiency, as Methylation slows, critical functioning breaks down, Methionine functions break down. This normally feeds the process with Biotin. As stated earlier, Biotin is critical to CO2 functioning, the exchange of toxins. As these break down, the body cannot clear the cells and toxins build. Adenosylcobalamin is known to effect the mucosal membranes. So without the process flowing, mucous can indeed build and functioning be reduced. This can be the explanation of why lung functioning decreases as disease progresses – as deficiency/inactivity increases. Fixing B12, especially as Adenosylcobalamin, along with ensuring working Biotin, may alleviate a lung function problem.
Cyanocobalamin – this is a synthetic form of B12 that has been used successfully for supplementation purposes in some cases. It is considered a more stable form and will not degrade as quickly when it sits on a shelf as opposed the bioactive forms. However, since it is synthetic, it requires additional steps for the body to convert it to make it usable. If the body is deficient in other critical elements, especially B2 and B3, it can prevent conversion. There are many cases in which people and animals have not been able to experience improvement utilizing this form of supplementation – especially in oral form. This would be particularly true if GI issues are already present. If you were directed by your doctor to take this form and have not experienced increases in your levels, or improvement in your symptoms, everything else I have described within this article can be contributing factors and bioactive forms should be considered.
I want to add one more nuance to treatment issues – especially when just supplementation of Methylcobalamin has been used and dismissed, leading to the statement that “B12” did not help so neurodegeneration in ALS has nothing to do with “B12”. Early in my research I came across a study article on ALSuntangled.com having to do with Methylcobalamin as a treatment. Though I understand that it was looked at “narrowly”, meaning the focus was ONLY on this form of B12, I later, with increased knowledge, found it odd that a B12 study would in no way reference any other form of B12, nor testing of related levels, in particular MMA. In my early research, not understanding what I do now, it made me dismiss a relation to B12 because I did not know better. I now understand that the study was woefully deficient since it did not explore all facets of B12 and its related gene mutations. Biotin, as of this writing, is also not a study on ALSuntangled.
One small conflict with high dose Biotin supplementation should be noted. Though high dose Biotin may indeed be a key to helping people, instituting moderation or breaks in dosing, or reduction in dosing after a period of time, should be considered. Biotin is known to share a protein transporter pathway known as SMVT (sodium dependent multivitamin transporter) in the body with 2 other elements. One is B5 (Pantothenic Acid), and the other is Lipoic Acid – both serving their own important functions in the body. In fact, this SMVT pathway may actually be a target of some drugs using the biotinylation method. SMVT is known to be a direct link to crossing the Blood Brain Barrier. The problem can be created that since so much Biotin is taken via supplement, that this transporter pathway protein could be overwhelmed and prevent the uptake of B5 and Lipoic Acid – creating a deficiency in these. Long term balance may then become important. After an initial high dose period, reduction in dosing should be considered and/or a “rest” day from supplementation every few days. Each body reacts differently. If you notice “other” symptoms after high dose use, this could be a factor and reduction or resting from dosing may be necessary even if positive results have been realized up to this point.
For anyone considering supplementation, even those who have a feeding tube, you should highly consider and discuss a well rounded liquid multivitamin with your doctor. Feeding tube formulas are meant to “sustain” a body in most cases – meaning they supply your daily recommended requirement of the basic nutrients. Whether you are still able to eat or if you are on a feeding tube formula, you may still be missing additional nutrients. This includes the additional elements that are explained further below. In order to “rebuild and repair”, it may be necessary to increase elements – just as someone who is healthy may do by taking a multi vitamin. Liquid, especially organic whole food versions, can provide easily absorbed natural forms of vitamins to provide extra support to the system. Again – please discuss this with your doctor to make certain any choices would be best for your particular situation. This should also include diverse forms of Probiotics and Prebiotics.
__________________________________________________________________________
Testing
If you or a loved one has a diagnosed MND (motor neuron disease) in particular, but also any troublesome autoimmune disease, you should check testing history to know if certain tests were run at any point in time during diagnosis. There is a possibility that if some were, levels did not yet trigger a cause for concern, or they were interpreted to be of no significance in your symptoms. It is also possible that medications, or progressing deficiency, have further drained nutrients, increasing symptom progression, and previous levels may not have reflected the worsening of symptoms. Additionally, as disease progresses, many doctors stress getting vaccines to make certain a patient is “less at risk” for certain illnesses. As stated in this article – these could “potentially” increase neurological and regular disease progression and leave a patient more vulnerable, so supplementation becomes more important after vaccination.
A few nuances to look for in testing:
If MMA was tested early in symptom progression, it may have been low or normal – masking any cellular issue with B12. Serum B12 could have been normal, high normal or even high during early diagnosis leading a doctor to rule out any connection to B12. Serum B12 is considered “normal” when it falls within a range that can run from 200-900 or even higher – that alone can give a doctor a false sense of assurance that it is not related to B12. A Serum B12 level could have also prevented a doctor from even testing MMA.
If Biotin deficiency (genetic, medication induced or dietary) was an underlying effect on MMA levels during testing, meaning inadequacies of Biotin would have kept MMA levels low masking cellular B12 issues, B12 would continue to deplete – symptoms would continue to get worse. If B12 was supplemented in any form, Serum levels could be normal or high normal, but neurological decline would continue. (this is why some patients and doctors state it is NOT B12 because they have been taking it and none of the symptoms improved – a false impression because other factors may be involved – which could have included other nutrient deficiencies)
As B12 further depletes and converts Adenosylcobalamin into Methylcobalamin to keep methylation functioning, those initially low MMA levels can eventually rise, even in the presence of Biotin deficiency. Without enough Adenosylcobalamin to convert MMA, the MMA level can naturally increase. However, if Biotin deficiency is still an issue, it can still keep MMA below “alarm” levels – again fooling anyone diagnosing for issues. Serum B12 can finally be entering the “alarm” stage if it is not supplemented – but MMA, even though beginning to elevate, may itself not be in an “alarm” stage because of insufficient Biotin functioning. (Biotin can still be effected by gene issues or medication intake that is keeping it deficient and effecting its functions. Biotin pathway disruption is keeping MMA low.)
Until Serum B12 falls into the extreme danger zone, likely below 250, the MMA level may still not be high enough to warrant action if Biotin deficiency (robbing/gene mutation) is a contributing cause. This would be of particular note to anyone on long term medication. Understanding that the medication itself could be causing the Biotin deficiency due to Avidin binding or pathway overload, means an MMA level cannot be trusted. Neurological symptoms in and of themselves should warrant supplementation of both regardless of diagnostic levels. Remember, Biotin-Avidin binding is used in serum testing and therefore any test result should be suspect and not relied upon in the presence of profound neurological symptoms.
If you have “HIGH” Serum B12 it more than likely means your B12 is INACTIVE. I have watched ALS patients post about Serum B12 levels above 900-1,000 stating their doctors, neurologists, have NOT been concerned. In fact, some doctors have told their patients that it is just a cause of the ALS progressing and it is normal. NO!!!! IT IS ACTUALLY CAUSING THE ALS TO PROGRESS!!!! At the very least, MMA should have been tested when this occurred. However, if Biotin is deficient, MMA – even if tested as Serum and Urine MMA – could still be within range. There is NO WAY for a doctor to know without genetic testing if you have a gene characteristic that means you are inefficiently recycling Biotin, causing low MMA, creating the high Serum B12. There is also no way without complete testing to know if that Serum B12 level is even usable B12. Many B12 deficiency patients have watched their Serum B12 levels fall into normal ranges when starting proper supplementation because they restarted cellular functions that were stopped, including toxin excretion, once the body had proper supplementation. Meaning they excreted the unusable B12 from the body.
If you have supplemented B12 in any form just prior to a Serum B12 test – that alone can cause high circulating levels of B12. In particular if you have Functional Deficiency. A doctor should know this and question it – but it is definitely not a standard thought process.
Some doctors have come to understand that other tests can help them assess the body from a chemically “functioning” standpoint. These include Organic Acid tests (OAT) and Hair Tissue Mineral Analysis tests (HTMA). A buildup of certain acids can alert them to Vitamins or Minerals that can be deficient in the body, or even at toxic levels and these will not show up on any standard Blood Panel (CBC or Chemistry). The only problem with those tests is that they cannot reveal functioning issues based upon gene mutations that simply keep the body at lower functioning capacity in some areas, possibly masking certain issues. This could include Biotin. However, they can go a long way to increasing the ability of a doctor to assess nutrient issues when diagnosing difficult cases. The problem is though that many doctors are not familiar with the tests nor how to interpret them, and they may not be able to even order them if insurance will not allow and a patient is unable to pay out of pocket as they can be expensive. And, certain areas of the country (US) or around the world, do not have easy access to these. Many labs require a doctor’s signature to obtain the testing, even though in almost all cases a patient ends up paying out of pocket for the test as insurance will likely not cover the costs.
For the sake of giving a general idea of tests that can reveal deeper issues, I will list various items that can be used in diagnosing “hidden” issues that can be causing disease and neurological decline. You can discuss these with your doctor to see if they can help to further diagnose a condition, to rule in or out additional items. Genetic testing for abnormalities for recessive genes (leading a body to less than optimal functioning) should also be considered for any issue related to Biotin and B12. Even though testing can elucidate the underlying problem, if testing is not available, supplementation of key elements can still be done to see if a body can be stopped from deterioration.
- Serum B12 – HIGH serum levels should NEVER BE IGNORED – they are a sign of INACTIVE B12 – Functional Deficiency – typically exceeding 700 but may register well above 900. Levels under 500 are suspect of Overall Deficiency and indicate severe when lower than 300.
- Serum MMA – for Neurological issues MMA (both Serum and Urine) should ALWAYS be run to gauge Adenosylcobalamin function – and determine how much kidneys are offsetting to keep blood levels low and prevent further toxicity. (low functioning/deficient Biotin could still prevent elevation in MMA, masking issues)
- Urine MMA
- Homocysteine
- HoloTranscobalamin (holoTC) – an active B12 marker
- Urine- 3-Hydroxyisovaleric Acid & 3-Hydroxyisovalerylcarnitine
- Plasma- 3-Hydroxyisovalerylcarntine
- Biocytin – this can be used to detect biotinidase deficiency. The enzyme biotinidase cleaves biocytin and makes it able to recycle biotin. Levels could therefore help to determine genetic insufficiency of Biotin activity.
- Propionic Acid
- Methylcitric Acid – not considered an accurate test for determining marginal Biotin status according to some studies. Therefore genetic insufficiency could be overlooked. Some OAT tests use this method to determine Biotin status.
- Biotinidase (BTD) gene/functioning (Low Functioning Possible)
- MUTase gene/functioning – (MUT-) is a rare possibility
- cblABCDEFGH gene/functioning – according to a study done in 2004, unidentified mutations of the “B12” genes in combination can prevent the body from properly converting B12 into Adenosylcobalamin. This would then become an increasing trigger in cases of diet change where Adenosylcobalamin is not being consumed from meat/seafood/eggs/dairy. These cases can signify why Adenosylcobalamin may need to be directly supplemented in order to bypass body conversion issues. (explaining why Methylcobalamin supplementation alone Would Not Resolve Issues, nor Hydroxycobalamin being able to correct decline) Low functioning levels of the required enzymes needed to convert B12 into Adenosylcobalamin, such as in the case of deficiency of nutrients needed to create those enzymes, could have triggered the body into decline. Again – all without any blood test revealing the deeper issue. To further this point, any professional reading this may want to read the following paper describing reactions for each B12 gene function. The paper refers to “late-onset” in many cases. To reiterate, “late-onset” means a body trigger was passed later in life, which still can mean a level of deficiency of a related nutrient failing to produce an enzyme/protein needed to complete the function: Genetic disorders of vitamin B12 metabolism: eight complementation groups – eight genes
- HTMA levels to detect Iodine / Molybdenum/ Selenium deficiency or other toxic levels (as a side note – Molybdenum in particular is connected to the proper conversion of toxic sulfites. Deficiency has been anecdotally linked to some cases of “ALS” because of a buildup of these sulfites. Deficiency has been noted in lowering ATP creation which would in turn create “mitochondrial dysfunction”. Molybdenum is also a necessary element in Taurine creation in the cell Cytosol, the deficiency of which has been linked to “DCM”.) **Any deficiency of these elements MUST be supplemented with great care as over supplementation can lead to toxic effects in the body. It should be done under medical guidance.
- OAT testing (Organic Acid) to detect a wide range of possible issues in nutrient functions.
_______________________________________________________________________
Vitamin Recycling and Muscle Wasting
For those who would like to understand more about issues with B12, I wanted to include additional information that could help you. Below you will find links to the websites created by Dr. Gregory Russell-Jones. His research allowed me to understand more in regard to why my dog reacted better to certain supplementation and even why I myself have had some continuing issues in my own metabolic functions. I encourage you to read through all of his websites to get information directly from one of the experts in this field. However, I thought it prudent to try and summarize some information that can help you to understand.
One of the biggest issues in B12 deficiency and in neurological disease progression, is muscle wasting – losing a tremendous amount of weight. I watched it happen with my own dog and have seen it happen in other animals and humans. I realized that the body was taking nutrients from its own muscle in order to sustain organ function – but why if I was providing nutrients? The likely problem was that there were still nutrients missing, or not enough of certain ones to overcome the body trying to restart chemical reactions. In particular this can happen when only one form of B12 is given such as Methylcobalamin. Hydroxycobalamin can be naturally converted to both Methyl and Adenosyl. Giving Adenosyl in addition helps to bypass any conversion step and provide the cells directly with a usable form that could prevent an additional strain on recycling Methylcobalamin.
On Dr. GRJ’s Autism website he refers to muscle wasting as being a link to B2 deficiency. B2, also known as Riboflavin, is a necessary component in recycling B12 in the body. Vitamins can “recycle” – meaning they can be used in reactions for a few times before breaking down and getting excreted. Much like you can reuse a tea bag for another cup, or your kitchen sink sponge until it gets yucky. Odd comparisons I know, but I am trying to make a point. B12 and Biotin can both function in this way but they will break down after a few cycles so a constant supply needs to be available to keep things functioning. A tea bag will become too weak to expel any flavor so a new one must be used – so too happens with some vitamins and minerals.
B2 is needed to recycle B12. B2 converts into 2 active forms, much like B12 converts into Adenosylcobalamin to be used in the Mitochondria of the cell and Methylcobalamin to be used in the Cytosol (liquid part) of the cell. B2 converts into FAD and FNM. Those forms require additional nutrients to convert them. (the “cycle” thing). In order to properly convert B2 the body needs a supply of Iodine, Selenium and Molybdenum. For those who have a history of Thyroid issues, Iodine may be a deficiency in your body. Depending on the foods you like or don’t like, or the diet choices you intentionally make such as avoiding meat, dairy, eggs or seafood, or even “gluten” meaning you avoid flours, yeast and fortified baked goods, may be why you could be deficient in certain items – including critical B vitamins, even Adenosylcobalamin. Yeast and Liver contain the highest concentrations of Biotin, Egg Yolk is next in line.
When you are missing certain vitamins and minerals – like B2 – it can mean that another vitamin may not be able to “cycle” in the body. If this happens – it may mean it can only be used in a limited way before getting excreted. That increases the need for the body to get more because it essentially “burns through” the on hand supply because it cannot “recycle”. Like when a child tries on a few different clothes items and even though they aren’t dirty, they throw them in the dirty clothes pile creating more laundry. Where does the body get more if a patient isn’t consuming more? From its own tissue – muscle wasting.
When I supplied B12 and a B complex to my dog she definitely improved – but there came a point when progress stopped – the B12 form was primarily Methylcobalamin though I did use cyanocobalamin too. I varied multi vitamins and diet items trying to understand what could help her and what didn’t. Because of the bouncing of nutrients I did provide her the missing elements at times in varied forms. When she got stronger she was able to eat better and that is when I directly gave her better natural whole food choices that improved her condition. But it is hard to understand the nuances as you are going through the process. Now, in hindsight, I have been able to put the puzzle pieces together. Biotin was a definite factor and how I came to understand this cycle, but B2 and its supporting elements played a significant role.
In the case of my dog, I also noticed significant improvement when giving her a combo liquid B12 that was just Adenosyl and Hydroxy. When giving her that form I noticed an immediate energy increase, but I also noticed vaginal mucosal discharge. As weird as it sounds, that signified that her body was using those forms directly and almost instantaneously to help chemical reactions. This could have meant that because she was missing additional elements needed in recycling other vitamins that were possibly necessary to convert Methylcobalamin, these forms went directly into the cell to stimulate functioning that had been dormant. Adenosylcobalamin is known to effect the mucous membranes. This is all anecdotal, but I just want to give as much information as possible.
When studying research papers and various articles on B12 and other nutrients you can find many conflicting or indeterminable summations. In fact, you can find many notations of “additional research is still needed to determine” when it comes to metabolic pathways. Experts STILL do not know everything there is to know about certain elements, including B12 and Biotin, and they can even disagree with others in their field. Perhaps that is why we constantly hear about doctors’ changing their “opinions” on why certain things may be good or bad for you. All you have to do is look to something like all of the studies and opinions on coffee to see the conflicting accounts.
_________________________________________________________________________
FDA WARNING
I must provide information regarding a warning of high Biotin use. It actually has NOTHING to do with adverse effects to the body, but rather the possible effect to any blood testing done. Because the medical bio-engineering community exploits the attraction of Biotin and Avidin in drug delivery, they also do it in testing procedures. Many lab tests, in particular hormone and cardiac enzyme tests along with Cancer Tumor Marker tests, but also Vitamin tests such as Serum B12 and Vitamin D, can be adversely affected by high Biotin content in blood. That means that results can be reported inaccurately, either high or low, and cause inaccurate medical diagnosis and treatment as a result. Avidin is used to bind to cells in the blood sample during testing and if circulating Biotin is high it can bind to Avidin and misrepresent the level of whatever protein/hormone/enzyme/vitamin they are trying to gauge. If you are supplementing increased amounts of Biotin you should notify your doctor for any specific testing such as cancer, thyroid, prostate or other hormones, or specific cardiac enzymes and vitamins. From personal experience, one of my own specialist doctors had NO understanding of this issue. Any abnormality that arises should be retested. Abstaining from supplementation for five days to one week for routine blood panels should help establish more accurate results. However, in emergency situations doctors should know of the possibility of an inaccurate result, especially heart related issues. If you are supplementing and feel it helps you, especially in very large dosages, it is also possible you could have a genetic abnormality that has been effecting you and perhaps caused inaccurate results for many years.
Since we know the Serum B12 test uses an Avidin-Biotin assay – we are relying on the results of a test used to measure one element without knowing if the other element used in the testing procedure is sufficient in the body. The test uses the “assumption” that Biotin, the very element that needs to be in adequate supply in the body in order for B12 to function properly, is actually in adequate supply. That is a HUGE ASSUMPTION. In essence that is a circular reference. In the early stages of symptoms, if testing is done on Serum B12 levels, and Biotin deficiency is causing Adenosylcobalamin to not be active, B12 can be reported inaccurately. It can actually come back high or normal because not every facet of B12 is actually functioning in the body and the body is circulating more to try and get tissue cells functioning again. At this stage it would be crucial to know if MMA was elevated or low in order to balance out the Serum B12 result by knowing if Biotin was sufficiently active or not – however, this too could be effected. It would also be critical to know if Biotin markers themselves are indicating deficiency – which could actually decrease MMA, hiding functional inactivation of B12. A doctor may interpret a low/normal level of MMA as having no connection to neurological issues because it is “masking” Biotin deficiency from diet or from genetic mutation.
Avidin could also be a wildcard in that if Avidin is in the blood due to medication or even consumption from egg white in some form, its pre-binding of Biotin in the body could also skew results. It would also become necessary to test urine and blood serum forms, though from research it seems that the Avidin-Biotin assay method is likely used in both areas and Avidin can get excreted through urine.
The other concern goes back to the “side effects” of certain medications. If a medication is stated to possibly alter “Lab Results” – this alone is a BIG FLAG that indeed it alters the Biotin pathways in the body – AND NO ONE IS PAYING ATTENTION.
To be accurate – this same thought process could be stated for any blood test that uses an Avidin-Biotin assay. If you do not establish that Biotin is NOT deficient in the body, then any test that relies on the “ASSUMPTION” may not be accurate. If the FDA can warn of over-consumption of Biotin, then how can it NOT state that deficiency could also be a contributing factor? I have no knowledge of how this particular testing method was adopted but it is an industry standard. I can only “assume” that there “should have been” testing done to establish accuracy within a standard Biotin range – but that could be a big assumption. Was that based upon repeated information from healthy people? Did they test everyone for a distinct Biotin level of some form before the assay was used to establish the levels? Does genetic “unrecognized” low functioning Biotinidase deficiency create additional issues? I am playing devil’s advocate in this questioning simply to make people, and any professional, think about the tests that are being relied upon to make “final decisions” on someone’s status. Those testing procedures may have been established before the ever expanding use of Biotin-Avidin binding in medications and vaccines, and the increased use of both. Hence the reason to question if anyone has taken this into account in modern day practice? A double edge sword in a world that relies on “we have always done it this way”.
For these reasons alone – a devastating neurological disease should NEVER be diagnosed without exploring all facets of Biotin and B12 testing, including all related metabolic functional indicators, and to test for any level of recessive gene mutations having to do with Biotin and B12 functionality that could now be a factor in deterioration. A disregard for knowing with absolute certainty that Biotin and B12 both as Methylcobalamin and Adenosylcobalamin functions, are indeed in adequate functioning amounts in the body, could mean the body will continue to degenerate without detection, when it could be caught and reversed before permanent damage is done .
Understand that many neurological diseases – in particular ALS (DM in dogs) – cannot be pinned down as to the start, a direct gene correlation, nor any true medication that can stop progression. That alone can mean that an unrecognized metabolic pathway can be overlooked based on many “assumptions”. The more I have researched B12 and Biotin, the more I realized how much is not actually known, admittedly by the researchers and authors of papers, and how much even experts differ when writing papers. Scientific papers and textbooks, including a 2015 edition on Nutrient Metabolism that I use, are filled with lines describing pathways as “yet to be determined”. Without understanding and exploring these nuances of Biotin binding and how standard Medications and Vaccines could be exacerbating the issue, and the way it can influence B12 all without detection, could be the link in explaining and treating ALS and other progressive neurological diseases, even autoimmune diseases.
If a medication is produced that uses the same pathway that is likely compromised in the first place – you can never fix the problem. Hence the reason the problem may be that researchers and doctors have made an assumption that it is NOT that pathway, the Biotin and B12 pathway, that is involved in the course of the disease. Clear research must be done on these factors alone before we can say there is no cure or explanation for a symptom progression. A neurologist MUST at the very least, test B12 and MMA. And even if tested and inconclusive in their view, should start a course of both B12 and Biotin, including using direct Adenosylcobalamin in addition to injection of Hydroxycobalamin, before dismissing their possible connection. But admittedly – this is MY Opinion.
From research, there have been studies started that are using extremely high dose Biotin to see if it effects neurological disease, in particular MS. However, from early information, it does not appear that the studies are dosing B12, in any particular form, at the same time. An absence of B12 supplementation, at least in the form of Hydroxycobalamin (though all 3 forms may be best), and the absence of supporting nutrients for cycling, would likely show very little long term positive response in testing models. (6/21/20- I have learned from MS patients that the amounts many are taking to alleviate symptoms are in the 100-300mg range – similar to the MD1003 study – and far above normal supplement dosing. The study did not appear to test for genetic biotin recycling issues (biotinidase deficiency), original Biotin deficiency, genetic B12 issues or deficiency, nor testing for MMA levels that could elevate with Biotin in the presence of B12 deficiency. Patients in general were not familiar with any direct connection between B12 and Biotin.)
The following post was made in response to a question about tumor marker elevation in Breast Cancer and if it could be connected to Biotin supplementation - not "caused by" Biotin use, but rather if it could have altered the results. In the case of the person who posed the question - after stopping Biotin supplementation for 7 days, their markers did indeed return to previous levels. The following response is from a doctor: The Endocrine Society in 2016 raised an alert that megadoses of biotin (also known as "Vitamin B7") could interfere with immunoassays that incorporate biotin and streptavidin - a bacterially derived biotin-binding protein- into their immunoassay design, and based on this the FDA issued warnings on biotin adverse interactions for a wide swatch of such tests, including: LAB TESTS 1. The Vitamin D (the 25(OH)D) test (false elevation) 2. Estradiol (false elevation) 3. Progesterone (false elevation) 4. Folate (false elevation) 5. Insulin (false low readings) 6. Luteinizing Hormone (false low readings) 7. PSA (false low readings) 8. Thyroid tests - TSH, T3, T4 (false low readings); thyroxine (false elevation) 9. Troponin (for cardiac infarction detection), causing false low reading, and subsequent patient death 10. Vitamin B12 (false elevation) 11. Others (testosterone, PTH, DHEA, FSH, HIV and Hepatitis A, B and C, HCG (used in pregnancy screens) and others) TUMOR MARKERS In addition, it can interfere - disastrously - as well documented by Amitava Dasgupta at the University of Texas, and cause inaccurate readings of tumor marker tests (which are biotin-based and rely on biotin to bind to the tumor antigen) for: • CA 15-3 (false negative, with 40% reduction reported) • CEA (mild reduction) • CA 125 (mild reduction) These are all false negatives and can therefore mislead into thinking that no significant increase in tumor marker occurred when in fact it did. SAFE TEST-DISTANCE TIME The half-life of biotin ranges from 8 - 18 hours, so that after one half-life has passed, 50% of the initial drug amount is removed from the body. More critically, the elimination half-life is estimated as 5 times the upper limit of (biological) half-life, meaning that plasma concentrations of the agent will be below a clinically relevant concentration and thus will be considered eliminated: for biotin therefore, that would be 90 hours (5 x 18), and we would add a 20% margin to handle slow metabolizers, bringing us out to 108 hours, ~4.5 days. CONCLUSION: Therefore, 5 days would represent the safest test-distance time, including allowing for differential in metabolism rate. So biotin should be discontinued at least 5 days before any of the immunoassay above, and most critical for tumor marker assessment. NOTE ON MEGADOSE: For biotin, a megadose is defined as 5000 μg (micrograms), equivalent to 5 mg, or higher. However, there remains a small but not zero possibility of some non-trivial interference from lower (non-mega-dose) supplementation, so caution suggests elimination of all biotin supplementation at least 5 days earlier than scheduled testing. Constantine Kaniklidis Director, Medical Research, No Surrender Breast Cancer Foundation (NSBCF) Oncology Reviewer, Current Oncology Member, European Association for Cancer Research (EACR) Society for Integrative Oncology (SIO) International Cardio-oncology Society, North America (ICOSNA) ORCID Profile: https://orcid.org/0000-0002-7043-5937
________________________________________________________________________
The Glyphosate Connection (Roundup and other Herbicides)
There are many Biotin dependent enzymes that are critical to life. Plants even have these enzymes and herbicides have been created to target specific ones in plants in order to kill off weeds/grass/etc.
Glyphosate was developed to specifically attack the Shikimic Acid pathway. This specific pathway is only found in Bacteria, Fungi, Apicomplexan and Plants – not in animals. The Shikimic Acid Pathway is composed of 7 individual steps/ chemical reactions – the first of which actually being a step that requires a Biotin dependent enzyme reaction called Phosphoenolpyruvate carboxylase. Supposedly glyphosate does not directly target this level. However, it is possible that glyphosate uses the entry into the shikimic pathway with an avidin-biotin binding technique to deliver the “drug” to the plant to attack the pathway. I have no direct information if this is indeed the case but it would follow a logical delivery system. Meaning that it could indeed also leave behind avidin residue.
Why is this important? Because we know that glyphosate has been found in human and animal tissue and even in urine excretion and has been connected to cases of cancer. Technically there is no absolute “proof”, just large amounts of circumstantial evidence. A Major Lawsuit has just recently been won based upon this connection. But how would it cause the problem? Though there are other chemicals mixed in with the glyphosate that are highly questionable, the direct answer may once again be hiding in plain sight.
Many popular cereal brands have been found to have high concentration amounts of glyphosate in their consumer end products. This is also the case for animal feed products. Meaning it has been absorbed by neighboring grains, vegetables and fruits during application in commercial growing. Glyphosate is even sprayed on non-organic wheat at harvesting to desiccate it for storage. Since glyphosate is designed to disrupt the same metabolic system that is found not only in plants, but also in bacteria, it means that when it is consumed by humans and animals through those same grains, vegetables and fruits, that it can then enter the intestinal tract and bloodstream and disrupt and KILL BENEFICIAL BACTERIA in the GI tract. Since glyphosate is also known to remain in animal tissue, it has been noted particularly to build in the liver, it means that meat consumption by humans and other animals can add additional amounts to the body and GI tract and expose it to the Good bacteria. That bacteria creates Biotin. If you destroy the natural ability to create Biotin, you form the basis for disease and cell mutation – cancer. The liver is the largest storage point for Biotin because it is needed to filter toxins – hence the reason the liver appears to retain the most glyphosate without the means to remove it properly because it has already destroyed Biotin producing bacteria – a vicious cycle.
If we never test Biotin levels because we “Assume” they can’t be affected, not realizing WHAT can affect them, then we will never identify deficiency or its further effect on B12. Additionally, if we “Assume” that genetic partial biotinidase deficiency should not be a big deal, we are disregarding everyday factors that could be disrupting low functioning Biotin cycling that can lead to Profound issues. All without easy detection by any standard blood test.
Since we know Biotin plays a critical role in toxin removal, the build-up of glyphosate in body tissue may be the result of Biotin deficiency caused by the continual ingestion of glyphosate and other forms of Avidin. Without Biotin supplementation a body, human or animal, may not stand at chance at recovery, especially if other factors, like medications and vaccines, add to the situation.
I will also restate the information I provided earlier in the article. In addition to glyphosate – GMO Wheat (and possibly other grain products) may have been altered to INCLUDE the Avidin Protein. A “double-whammy”. This means that the grain products may not only have glyphostae, BUT ALSO directly contain Avidin. Might this double barreled approach be the link to “celiac” issues and the increasing amount of GI Tract issues in addition to various disease?
As stated earlier in article: The Avidin Gene is now being introduced into wheat crops. This is done to prevent damage from insects during storage – eliminating the need to spray them with glyphosate or other products – the “killer” is INSIDE the wheat. The following study proved not only that Avidin protein was built up in “treated” wheat, but that it transferred into the insects. This would mean that the very same thing could happen in humans and animals consuming these products. The reaction would not be immediate like in the body of an insect. However, with constant consumption of “grain products” (breads, cereals, crackers, cookies, pizza dough, or anything that uses wheat flour in its production) – every being would be at risk for Biotin deficiency as the Avidin protein is constantly introduced back into the body. As of this writing I do not know if this genetic process has been introduced into other plant based flours, but it is likely the next step.
https://pubmed.ncbi.nlm.nih.gov/26194497/
________________________________________________________________________
Pet Owners
If your pet is experiencing any neurological issues, walking issues and weakness, skin conditions, laryngeal weakness or paralysis, megaesophogus or a history of pancreatitis attacks, liver and kidney problems, diabetes, cushings, thyroid issues and even heart issues, Biotin and B12 deficiency can be at the heart of your companion’s issues. The medications and vaccines that they get are made the exact same way as human forms so the pattern of deficiency can follow the exact same path. I believe Biotin is even more critical in animals than realized, especially based on the increase in skin conditions. Animals go through coat changes all year long to prepare for seasonal changes so their body has a higher demand for cell turnover, making them more susceptible to deficiency.
If you feed raw or natural food – check your food labels. Even if you are not directly feeding whole raw egg regularly, processed raw, dehydrated or freeze dried food can contain whole raw egg, chicken or duck usually. Even if you are not feeding raw or whole egg, your food simply may not supply enough Biotin and B12 to overcome general nutrient demands and to offset vaccines and medications. Processed food, kibble, can destroy natural B12 and therefore must add the synthetic form that may not be able to be converted by the depleted system.
There is very strong thought that whole raw egg should not be a problem for dogs since they would eat eggs raw in the wild. But wild dogs would never have a continuous supply of eggs in the wild. They would eat the animal long before they would consume an egg a day. In addition, a wild dog would consume a whole animal including organs and gut bacteria that would help to overcome Avidin consumption. And most birds in the wild have a “mating season” so continual supply would usually not exist. In winter months a wild dog/animal would likely not have access to eggs, allowing the body to rebuild and fix itself from periodic deficiency. They obviously would also not battle vaccine and medication issues adding to problems in the body.
The other nuance is if gene issues do play a part in dogs – and this could be the connection to certain breeds being more vulnerable. I am still in search of any specific studies on gene related biotinidase deficiency noted in animals. (gene mutations that could lower biotin recycling in cells). General Biotin deficiency and B12 deficiency has been noted and studied – in particular when intentionally induced. But genetic predilection for the issue, like in testing human babies, along with specific B12 related gene abnormalities, may not be widely studied, if at all.
As of April 2021 it is now listed that the BTD gene has been isolated in canines - this is related to Biotin/Biotinidase issues as I have described throughout this article. In FACT - BTD has been isolated in 346 organisms. Gene isolation alone does not yet reveal extensive study on the matter of identified deficiency or low functioning issues in canines and its connection to disease, especially sole neurological issues such as DM, but it provides a starting point. When I first released this article in April of 2020 I sent it to a few researchers (in both the human and animal worlds) questioning the connections I had made - inquiring if anyone could elaborate on research in this area. Not surprisingly, I did not receive a response. However, listing of the gene isolation does prove that animals could then be subject to the exact same sensitivity of deficiency and may then need to make certain to avoid extended exposure to elements such as raw egg white, and, may need certain increased levels of intake in regular diet or specifically in disease and during treatment with medications, especially antibiotics. It could also then explain deterioration in relation to annual vaccines or anesthesia events. I am also in the process of investigating how an issue known to the use of Ivermectin in many of the same breeds who are prone to DM (Shepherd, Corgi) and even Border Collies (known to be prone to B12 deficiency) might be further related to this very same Biotin/B12 connection.
I have had heated discussions with owners who have fed whole raw egg to their dogs on a continuous basis for years and claim to have never had a problem, so therefore they implied that my information has to be wrong. To them that means they can say it is safe for ALL other dogs. That would be like stating you can eat peanuts so there is no basis to how another person can die from just touching them. One owner who made this argument made a point of stating their dogs never had any skin conditions – as if that was the only problem with Biotin deficiency. I asked if they could tell me what their dogs finally succumbed to at the end. One dog was hypothyroid from the age of 5 and on meds for his whole life (hypothyroid and B12 deficiency often go hand in hand), another had heart issues that were noted later in life (another B12 connection), and yet another had a history of GI issues, but yes, they did state that 2 other dogs never had “any” issues which I can only assume means no diagnosed long term disease. Though they did admit not all of their dogs consumed the same amount of eggs on a regular basis. I do not know the breeds, sizes, or any other history and overall diet. In another discussion with an owner, they too stated NO problems with whole egg consumption – no skin conditions. However, their dog did experience an ACL tear which can mean an underlying tissue weakness from deficiency.
We can agree to disagree if you are someone who feels this recommendation absurd. But the SCIENCE of how Avidin could bind all of the Biotin in a raw meal containing whole egg, or a preground raw food mixture containing egg, exists, leaving it unavailable for the body to use. Biotin binding inside the body, leading to undetectable deficiency related problems, is a “long term build” issue when low levels are continually consumed (not an overnight one) that can eventually break down cellular function leading to various disease, all under the radar if the body cannot resupply and support the deficiency. The case also remains that Avidin can rob Biotin from places such as bone marrow and lead to the start of any number of issues and cancers. The misunderstanding is that large quantities must be consumed to be a problem. But just like other toxins, yes a large quantity can cause a problem in a short time frame, but continuous smaller dosing is how it can affect cell function over a period of time, eventually leading to a visible symptom. (heart disease is not always visible, cholesterol level increases and liver function issues are not always visible, cancer is not visible until it may become life threatening, etc.) And please keep in mind – the smaller the animal, the more at risk they can be from the consumption of a whole egg. One owner cannot say it is safe for all dogs, when they have no idea what another owner provides as a continual diet that could risk supply of additional Biotin or eventual B12 issues, nor to know if gene issues could make another dog more prone to deficiency sensitivities. Puppies may also be at higher risk for issues, especially if they were the “runts” of a litter, meaning they may not have built up a good body supply of any particular nutrient. Additionally, a growing body should not risk having anything block the known functioning of nutrients, fatty acid metabolism being critical.
I am simply suggesting that if your pup is having issues, skin, yeast, digestive, neuro, organ, hormone, heart, muscle/ligament or otherwise, that you abstain them for all raw egg white (yolk is acceptable and very beneficial especially because it contains B12, Biotin, Selenium, Iodine and Molybdenum among many other nutrients). This advice includes any premade food (raw, dehydrated or freeze dreid) that would supply it daily. You would need to test this for at least 3 months or longer, in order to see if symptoms begin to improve. A body has a natural pattern of cell regeneration, blood being 120 days, GI tract cells being 3-5 days as they shed, etc. So to fix and improve what may have gone wrong, can take an extended length of time before you see the benefits. You may need to increase supplementation with a quality B Complex during this time to replace what the body has lost – functioning that has already been effected. I only came to understand Biotin issues when I used a highly touted US made pre-ground raw food that contained whole raw egg. Up until then my dog was essentially recovering from deficiency and improving her neurological status. The downturn came quickly after starting the food, and only more research is why I now know what I do and try to warn others.
As I wrote in the article on my DM dog, fish oil supplementation also had an adverse effect on her neurological symptoms. It was recommended by the vet to increase fish oil to help with what was assumed to be allergy and arthritic issues – in addition to cognitive issues. When I noticed it appeared to increase her symptoms I was confused until my research brought me to understand that she could not properly process an increase in fatty acid due to the missing nutrients involved in fatty acid metabolism. This one point in my article connected with many people who saw the same issue with their dogs. If you force the body to deal with a higher intake of fats it can drain resources quicker.
After writing that original article I heard from many owners who saw very positive results in their neurological/weak dogs after starting intense supplementation of Biotin and B12 along with B Complex. Many were in early stages of deterioration so symptom reversal was easier. And yes, I did hear from owners who admitted that a year after adding whole raw egg to the diet a few times a week, is when they noticed the hind end weakness typical of “DM”. The additional trigger appeared to be symptoms starting within a few months after vaccination. That connection would click as it would have increased stress in the Biotin pathway affecting Antibody production.
Though this post contains all of the updated information, and the connection to vaccines and medications that can play a part in neurological deterioration, if you would like to read through the original DM article, it is linked below. That article stepped through my experiences with my DM dog, including information on her symptom progression and contains some specific information in respect to dogs that can be helpful to anyone with that particular concern.
__________________________________________________________________________
NOT SELLING ANYTHING
This article was not written to “sell” you anything. I have gained nothing from any source to put all of this information in one place. The hundreds of hours spent on this writing and research is all done in hope that it will reach someone who needs to see it – change someone’s life for the better. What you do with the information is completely up to you.
I am also not trying to give anyone false hope. I wanted to provide people information that I collected over the past 3+ years that I was never able to find all in one place. You don’t know what you don’t know until you find out something new. Researchers test things in a very narrow environment and never seem to relate their results to something else – so I started to connect dots as I read more. And I can guarantee you that most doctors out there do not know these nuances. And the ones that might – simply don’t realize how many people need to understand how it could relate directly to their circumstance.
Remember, for ALS in particular, there is no absolute drug that can truly help. Perhaps it is because most of the medications work in the same metabolic pathway that is breaking down and they could then only make the issue worse. This can even include the failure rate of stem cell treatment because those cells need nutrients to proliferate and repair damage. For other neurological diseases there may be slight differences in their progression meaning certain drugs have helped in some small way. So if diagnosing and treating ALS and DM has been a mystery all these years, just maybe, the very things I described, hold the key to why it has not been recognized. The answer has been hiding in plain sight.
__________________________________________________________________________
WEBSITES Of INTEREST
The following are links to the websites created by Dr. Gregory Russell-Jones. Dr. GRJ is an Australian researcher specializing in B12 and is the creator of Transdermal B12 Oils, an alternative delivery system to injection.
The link below to his B12oils website will bring you directly to a page for what he calls “Paradoxical B12 Deficiency”. He describes the case of “HIGH” B12 levels in relation to B2 deficiency, along with its related necessary nutrients of Iodine, Selenium and Molybdenum. Paradoxical Deficiency is equivalent to using the term Functional Deficiency. It is however still possible to have Functional Deficiency be caused from Biotin Deficiency and why Biotin markers and/or Gene defects should be tested to understand if it is playing a critical part.
Regardless of cause of Functional/Paradoxical B12 Deficiency, HIGH Serum B12 levels Should NEVER BE IGNORED. If you are experiencing neurological issues, B12 Inactivity/Deficiency is ABSOLUTELY CAUSING the problem and MUST be resolved to prevent permanent damage.
- http://www.wipeoutautism.org/
- http://preventingdementia.org/
- https://b12oils.com/paradoxical.htm
- http://www.vitaminb12deficiency.info/
- http://www.vitaminb12deficiency.net.au/
__________________________________________________________________________
This video contains information most people do not understand about B12. It explains how Folate can mask B12 deficiency by correcting Macrocytosis, the element medical professionals were trained to look for as an indication of B12 deficient anemia. It also explains how anemia is the LAST sign of progressing deficiency. The video depicts 4 totally different progressions in children and adults and discusses other case progressions. One depiction is of a Pediatrician, a medical doctor who was himself dying from B12 deficiency before a test actually revealed his level of deficiency. Experts explain many of the pitfalls and assumptions made when dismissing B12 as a related factor in neurological, psychological and physiological disease progression. Diagnosing and Treating Vitamin B12 Deficiency https://www.youtube.com/watch?v=QqjyAeOLyKM
______________________________________________________________________________
Various Writings Reviewed For, or Related to, Article Content
- Could It Be B12?: An Epidemic of Misdiagnoses – book written by Sally Pacholok
- Misconceptions about a B12 deficiency
- The Many Faces of Cobalamin (Vitamin B12) Deficiency
- Time to Abandon the Serum Cobalamin Level for Diagnosing Vitamin B12 Deficiency
- Functional vitamin B12 deficiency
- Biotin Deficiency Inhibits Heme Synthesis and Impairs Mitochondria in Human Lung Fibroblasts
- BIOTIN SAMPLE
- The Link between Nitrous Oxide Uptake and Vitamin B12 Deficiency
- Organic Acid Metabolism
- The Effect of Vitamin B12 Deprivation on the Enzymes of Fatty Acid Synthetis
- Vitamin B12 Deficiency and its Neurological Consequences
- Low vitamin B12 levels may lead to brain shrinkage, cognitive problems
- Vitamin B12 status and rate of brain volume loss in community-dwelling elderly.
- Functional cobalamin (vitamin B12) deficiency: role of advanced age and disorders associated with increased oxidative stress
- Detection of functional vitamin B12 and folate deficiencies, while serum levels are normal
- Biotin deficiency enhances the inflammatory response of human dendritic cells
- Interrelationship of Vitamin B12, Androgens and Cortisol in Chronic Stress and Associated Vascular Dysfunction
- https://www.b12deficiency.info/home
- Neuroenhancement with Vitamin B12—Underestimated Neurological Significance
- Coenzyme B12 (cobalamin)-dependent enzymes.
- Methylmalonic and Propionic Acidemias: Clinical Management Update
- Human ATP:Cob(I)alamin Adenosyltransferase and Its Interaction with Methionine Synthase Reductase
- Genetic disorders of vitamin B12 metabolism: eight complementation groups – eight genes
- A curated gene list for reporting results of newborn genomic sequencing
- Navigating the B12 Road: Assimilation, Delivery, and Disorders of Cobalamin
- Holotranscobalamin, a marker of vitamin B-12 status: analytical aspects and clinical utility
- 3-Hydroxypropionic Acid and Methylcitric Acid Are Not Reliable Indicators of Marginal Biotin Deficiency in Humans
- Urinary Excretion of 3-Hydroxyisovaleric Acid and 3-Hydroxyisovaleryl Carnitine Increases in Response to a Leucine Challenge in Marginally Biotin-Deficient Humans
- Biological functions of biotinylated histones
- Mitigating effect of biotin against irradiation-induced cerebral cortical and hippocampal damage in rat brain tissue
- The enzymes of biotin dependent CO2 metabolism: What structures reveal about their reaction mechanisms
- https://b12awareness.org/
____________________________________________________________________
A movie was made about Sally Pacholok – writer of “Could It Be B12?: An Epidemic of Misdiagnosis.” The above documentary features her. Though the below is a theatrical presentation, it does have some additional “medical” depiction and references for B12 deficiency that some may find of interest. Sally Pacholok has Pernicious Anemia.
If you would like to contact the Author of this article directly you can use the following link: CONTACT

Thank you for this FASCINATING research and great critical thinking! You put much time into this and are truly passionate about sharing what you have discovered and it is much appreciated! You provided so much food for thought, I have no doubt I will be referring to this often. After reading, I started with trying to find out more about avidin sneaking into our food without us realizing we are ingesting it. Came upon this and thought you would be interested – Development of Transgenic Wheat (Triticum Aestivum L.) Expressing Avidin Gene Conferring Resistance to Stored Product Insects
Abstract
Background: Wheat is considered the most important cereal crop all over the world. The wheat weevil Sitophilus granarius is a serious insect pests in much of the wheat growing area worldwide and is responsible for significant loss of yield. Avidin proteins has been proposed to function as plant defense agents against insect pests.
Results: A synthetic avidin gene was introduced into spring wheat (Triticum aestivum L.) cv. Giza 168 using a biolistic bombardment protocol. The presence and expression of the transgene in six selected T0 transgenic wheat lines were confirmed at the molecular level. Accumulation of avidin protein was detected in transgenic plants compared to non-transgenic plants. Avidin transgene was stably integrated, transcribed and translated as indicated by Southern blot, ELISA, and dot blot analyses, with a high level of expression in transgenic wheat seeds. However, no expression was detected in untransformed wheat seeds. Functional integrity of avidin was confirmed by insect bioassay. The results of bioassay using transgenic wheat plants challenged with wheat weevil revealed 100 % mortality of the insects reared on transgenic plants after 21 days.
Conclusion: Transgenic wheat plants had improved resistance to Sitophilus granarius.
https://pubmed.ncbi.nlm.nih.gov/26194497/
LikeLike
Wow – THANK YOU for the link. This actually fits perfectly with why “Gluten” issues could be tied to Biotin if this process is in mass production. There has been thought that celiac issues can be of an alternate cause – some of which being tied to Glyphosate (of which I added a section to the article apparently after you made this comment – glyphosate being capable of killing gut bacteria when consumed from cereals and other products). I need to try and find some more information on this and see if it is in any regular use as it can be a missing link in how humans and animals are having increasing disease issues. Your linked article was written in 2015 so if this is in production it could be another reason why there is such an uptick in celiac issues and in related animal disease. What is interesting is that for non-organic wheat they do spray it with glyphosate to desiccate it. Glyphosate may use an avidin-biotin binding technique that attacks the first level enzyme reaction in the shikimic acid pathway to infiltrate the grain. Thank you so much again for the link, and Thank You for your kind words on my efforts.
LikeLike
Pingback: B12 and Its Possible Role in Whipple Procedure Recovery – Being Thankful For